Aside from a progressive loss of the social mindset, our condition manifests with several other neurological and physiological features.
One of these is a direct result of our megalencephaly and consists of significantly increased verbal, memory and learning ability.
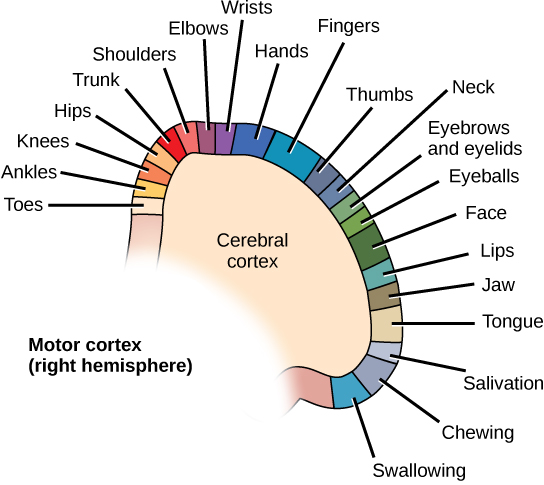
Two more features are linked to hyperactivity of the dorsal anterior cingulate cortex and consist of obsessive–compulsive disorder–like behaviours and significant motor symptoms, most notably swallowing difficulties and, in my case, tic disorder.
A fourth feature is likely the result of hyperactivity of the posterior insular cortex and consists of sensory hypersensitivity involving sight, smell, touch, taste, pain and temperature.
In addition to these features, I have anatomical, gastrointestinal and endocrine features in common with conditions linked to overactivation of the RAS/MAPK pathway, a signalling pathway associated with autism with megalencephaly, which is discussed on Genetics of our lack of the social mindset.
Our condition also has an apparent contribution from our paternal family histories.
Like the sections of Presentation and progression of our lack of the social mindset, this page contains many excerpts of dialogue between me and my friend that may offend some social-mindset sensibilities, however they are included for clinical and neuroscientific relevance, to aid in understanding how we think. Try not to take them personally, and do not attribute intent to harm where there isn’t any.
Language, memory and learning
Both of us are hyperlexic and have increased semantic memory and a propensity to go on research sprees.
I was recorded to have said my first word at 6 months of age (typical: 1 year[1]). My father stated that I was ‘very advanced with [my] talking’ and ‘spoke adult at the age of 2.’ My mother stated, ‘You were good at it, which is bizarre for autistic people.’ The father of a family friend had told my father that, as a toddler, when he spoke to me, it was ‘like talking to an old man’ and that I ‘used long words and grammar and context and idioms and complex sentences’.
I had significant echolalia as a toddler. Even though I would speak unprompted to my parents and was very talkative, I usually repeated questions they asked me back to them rather than answering them.
At age 4, my friend completed puzzles with 1,500 pieces and had memorised the times tables up to 13.
At around age 8, I became interested in the longest words in English and had memorised over a dozen of them. I also memorised the longest word in Greek, which was 183 letters long, and became known for this at school and would be asked to say it to people.
At age 8, my friend was able to correctly answer 20 simple maths questions (such as 7 x 4 =) in 14 seconds, equating to one every seventh of a second.
At around ages 8–9, I kept lists of words and homophones in a scrap folder to remember them. At around the same ages, I was interested in palindromes, ambigrams, optical illusions and drawing mazes and intricate geometric patterns. I also memorised most of the details about the planets of the Solar System, such as orbital periods, rotation periods and natural satellites.
At age 9 or 10, my friend increased his record for the previously mentioned maths task to 10 seconds, equating to one correct answer every half a second.
At age 10, I became interested in Windows commands and tricks. At school, I figured out how to send a custom popup message to every computer in the local area network (the classroom) at once using cmd. I later told my friends and a few others how to do this. A year assembly was held over this issue, and my friends and I received detentions for this (my only one at this school) and were accused of ‘hacking’. Although I did not repeat the act after this, the technician tried to block cmd, but I showed him that I could recreate it using Notepad, so he then tried to block Notepad, but I showed him that I could just right-click and create a new text document, after which he gave up.
At around age 11, I memorised the digits of pi to around 190 digits. This was increased to around 424 at around age 15. At age 15, my friend memorised around 110 digits of pi in 10 minutes.
At age 11, inspired by a technically skilled friend at school who had his own, I purchased my first shared hosting plan, installed WordPress and ran a website featuring a chatroom and forum.
At age 12, I temporarily memorised the binary for ASCII.
At age 13, when I acquired my first smartphone (an Android), I learnt how to root it, unlock the bootloader and install a custom ROM. I would install root-requiring mods and apps that would block ads and add customised functionality that would be beyond the limits of native apps, such as disabling read receipts in messengers.
At age 13, I made written lists of uncommon or archaic words in a notepad in order to remember them.
Between the ages of 13 and 15, I embarked on a massive research spree of aviation, memorising most of the common or well known aircraft models and some less well known, their rough years of production and service and numbers produced. I also memorised almost all major aircraft accidents, including their causes, rough dates and numbers of fatalities.
Immediately after leaving secondary school, I suddenly embarked on a massive research spree that began with politics, ideologies and architectural movements before moving on to world history, early hominids and language families and linguistics. I memorised the national anthems of a few dozen present and past countries, some of which I memorised the lyrics of, others the ability to play the music on piano and others both.
At around age 15, I learnt the Cyrillic script. At around age 16, I successfully memorised the Malayalam script but soon forgot it due to lack of usage. The same occurred with the Tifinagh script at around age 17. I learnt the Korean script at around age 17 and continue to be able to read it to this day. I also memorised almost all of the Arabic script at the same age. Through Wikipedia-reading, I passively learnt the Greek script and the Latin orthographies and phonologies of over a dozen mostly European languages. I also passively learnt almost all of the International Phonetic Alphabet.
At age 16, my friend began a research spree on German verbs. This resulted in him knowing almost every verb in English and German, due to having had extensive activity on a German–English dictionary and translation website, where he became one of the top-contributing users. He also compiled a spreadsheet dictionary of around 30,000 German verbs. He soon learnt the Cyrillic, Greek and Arabic scripts and world history after myself and also studied prehistoric archaeological cultures. At around ages 17 and 18, he increasingly studied maths and became proficient at calculus.
At age 16, my friend gained membership of the high-IQ society Mensa via scale 3 of the Cattell Culture Fair Intelligence Test, with scores of 137 on form A (99th percentile) and 144 on form B (97th percentile).
At age 17, I began a research spree on human genetic haplogroups (in particular, Y haplogroups) and the precise migration patterns of humans out of Africa.
At age 17, due to my research habits, I had accumulated 4,774 tabs in my Google Chrome browser. I had modified my browser with extensions to accommodate this many tabs without running out of memory, to facilitate these habits. To this day, I continue to accumulate hundreds of (or over a thousand) tabs every session, though I have not reached 4,774 since.
At ages 18 and 19, I attempted the number memory test at humanbenchmark.com,[2] which tests the ability to remember increasingly long sequences of numbers shown temporarily on screen. Both times, I reached 14 digits, which placed me in the 97th percentile.
At age 19, I attempted the verbal memory test at humanbenchmark.com,[3] which shows words in succession and tests the ability to recognise a word as having previously been shown. I reached 239 words, which placed me in the 100th percentile (i.e. the highest score on record at the time). My friend later also attempted this test and reached 235 words.
At age 19, I began a research spree on taxonomy and memorised the rough taxonomical relationships of most organisms. I then began in earnest my research spree on genetics and genetic diseases.
At around age 19, my friend began a research spree on Intel CPU microarchitectures and the Windows NT kernel and became proficient in C++. I only became competent at coding (JavaScript, CSS and PHP) immediately prior to building this website.
At age 19, my friend began a research spree on telecommunications and came to extensively understand the exact paths and exchanges that mobile and Internet signals take.
At age 20, my friend began a research spree on dentistry and became proficient in areas such as anatomical nomenclature and dental formulae.
At age 20, my friend began a research spree on theoretical physics, learning concepts such as Lorentz–Minkowski space, pseudo-Riemannian manifolds and frame-dragging.
At age 20, I extended my genetics research into much of human and animal biology and began my research spree on neuroscience, studying most regions of the central nervous system.
At age 20, I attempted a one-minute typing-speed test and achieved an average speed of 122 words per minute. My friend performs at speeds approaching this figure. The population average is reported to be 40 words per minute.[4]
Both of us continue to digitally save any rare or archaic words we did not know the meanings of.
At age 22, I stated:
‘An IQ of 80 [~8th–10th percentile] is already borderline intellectually disabled, just like an IQ of 120 [~90th–92nd percentile] is already borderline gifted, which seems weird but is just how it is.
Anything just above 100 is already 40 less than us, so it’s already astronomically dumber. We’re just that much higher above everyone else.
So the massive peak that clumps around 100, what should appear “normal” to us, as it’s portrayed, is actually extremely dumb compared to us, so even people we consider extremely dumb will have 100 IQs.
That’s just how it is; that’s how the world looks from our perspective. 80 and 100 compared to us is nothing; the distance between them is less than between average and us.’
Learnt anxieties/OCD
We both have learnt, post-early-childhood anxieties that take the form of behaviours similar to those found in obsessive–compulsive disorder (OCD), which I am diagnosed with, as mentioned on Background.
However, we are not distressed at the fact that we have the behaviours, nor do we consider the thoughts ‘unwanted’, and as such, it is debatable whether they constitute the diagnosis of OCD as clinically defined, which requires such distress.[5][6]
Additionally, the behaviours appear to be a result of our condition rather than a standalone condition. They fall in line with a far greater weight placed on innate survival goals over the social mindset within the context of a greater rate of learning. A diagnosis of OCD requires that the behaviours are not better explained by another disorder.[5]
OCD behaviours have been linked to hyperactivity of the dorsal anterior cingulate cortex. The explanation for why our OCD behaviours do not involve distress and why the clinical definition of OCD includes such distress is found in this block.
A 2013 meta-analysis found that OCD symptoms tend to cluster in four groups: contamination/cleaning, symmetry/order, hoarding and forbidden thoughts.[7]
Germ avoidance
Both my friend and I have significant infection-avoidance procedures, though most of them have become subconscious habit. They increased in line with our increase in knowledge and thus generally followed the progression of our loss of the social mindset, being minimal in early childhood and steadily increasing into adulthood.
They include, but are not limited to:
- inspecting, washing or avoiding cutlery and crockery
- using tissues, clothing or uncommonly used body parts to touch surfaces
- controlling our breathing when passing through certain indoor spaces.
They are elaborated below.
At age 11, there was an instance that I later recounted at age 19 as follows:
‘I got reminded for the first time of an instance in Year 6, absolutely ridiculous one, where we were in that garden in the photo I sent you for an outdoor skills lesson, and at one point, everyone was sat in a circle, and the teacher made us try this soup, and it was in one cup, which he passed around, and when it got to me, I refused. I’m not sure if it’s right, but I seem to also remember stating why I refused.
But either way, it got the whole class just staring at me and the teacher annoyed, and because it was year 6 and because of that, I reluctantly had to sip from the cup. I was very lucky not to get an infection. It was a considerable conflict with the teacher before I finally let up. He was way more annoyed about it than he needed to be.’
My friend replied, ‘I also would have done at that age, certainly, even before then. That was the first manifestation of my behaviours in this area. I’ll have to ask my mum when the signs started, because I wouldn’t eat off of restaurant cutlery, and I wouldn’t drink out of a cup without a straw, as long as I can remember, definitely at a very young age, and it made me feel sick, and I wouldn’t kiss family members, and I wouldn’t eat off of something they had eaten off of.
I don’t drink out of glasses at home. I have a straw. It started immediately, the refusal. My nan and mum still buy straws for me lol. It’s been a common tradition, because they know my behaviours. They’ve always laughed at it, though. It’s been a common theme.
I just couldn’t drink out of a glass that someone else has had their lips against. I just can’t. It doesn’t matter who it is, unless it is a girlfriend that doesn’t have a cold.’
At age 12, a girl from my previous school private messaged me asking to go out. After rejecting, I stated, ‘You know that horse in your profile picture? Was it like a wild horse not kept in stables, or was it a clean one? Because if it was left to roam, it would have parasites, and they could kill you if you pet it then not wash your hands.’
At age 14, in an answer to an online Q&A question about what habit others have that annoyed me the most, I stated, ‘Putting any random object, or their hand, in their mouth. It’s disgusting.’
At age 14, I stated that I ‘always try not to inhale certain air deeply or through my mouth’, ‘always use certain fingers for eating and other fingers for other activities’ and ‘always wash my hands before eating anything I’ll have to physically touch’.
At age 15, I stated to my girlfriend at the time:
‘When I make a hotdog … I never touch the hotdog. I use the plastic of the container or a fork to touch it, and I only wash my hands right when it’s ready on the table.
You might ask, well why don’t you wash them before that, so you can touch it instead of using forks? Yeah, well then I will touch the plate to move it to my table, and that will mean I have to wash my hands again, which is waste of time and effort.
When I use the tap, I never touch the knob with my fingers, only the back of my hand or little fingers. Same when I dry my hands; I never dry my index and thumb fingers, so that I can hold my hotdog without [contaminating it].’
At age 16, my friend stated:
‘I cannot eat off of cutlery very well, and I have to use straws; bacteria reasons, because someone else has in the past. It has been in someone else’s mouth. I have my own glass. I have not been ill in a very long time.’
I replied, ‘I wash every fork and knife under the tap before using, and I only ever hold the handle.’
At age 19, I stated:
‘I eat with a spoon or fork every time. I haven’t eaten using my hands in several years now. I use a bowl or plate and cutlery for everything; cookies: 6 in a bowl with a large spoon to lift.
I guess I don’t use cutlery with chocolate bars, because they’re wrapped, but I make sure the chocolate never comes so far out of the wrapper that it will touch a surface when I put it down.
Everything is thought out; at least, it was. Now, it’s a subconscious habit. I don’t think about this anymore at all. It just happens. I see my mum freaking out at my practices, and I don’t know what I’m doing weirdly.
The time I got ill in February 2008 was almost certainly from rolling around on the floor of the main hall of my primary school and then eating toast by hand that was offered by the staff. The timings and actions correlate perfectly. There was something going round clearly, because only the next month in March, that boy threw up in my class.
So I practically never eat by hand since then, unless I thoroughly wash my hands, but I never waste my time with that usually, just use cutlery.’
At age 19, I stated, ‘Oh, now I don’t wash my hands to hold a hotdog. I use cutlery only. I impale a fork at a 45° angle through it and lift it using the fork.’
At age 19, I stated, ‘I look at the insides of glasses and cutlery and crockery just like you, sifting through them until I find a spotless one.’
At age 19, I stated, ‘I cannot use tissue boxes, because my parents don’t buy them, because I went through them too quickly. I’ve been using toilet rolls as my main bedroom tissues for 2 years at least.’
At age 18, my friend stated, ‘I can’t use cutlery. Makes me feel sick. That’s why I have plastic cutlery and use a new one each time. I can’t eat off of anything that has been in anyone else’s mouth.’
At age 20, I stated:
‘Sister still coughing. For god’s sake, when will it stop?’ My friend replied, ‘Don’t want to know.’ I replied, ‘I was about to [get food] until she manoeuvred down the hallway, transported her ill self down the hallway.’
My friend replied, ‘Put new clothes on; get another set of clothes, and use that to tie round your mouth and nose; put another shirt over your head, and close your eyes whilst walking along; open them fractionally to get the food; return; remove the gear. Also, get hand sanitiser so you don’t have to use the bathroom soap, the bathroom that she uses.
But yes, I’d hate that situation, because it would cause me to take these time-consuming, inconvenient measures, all because of her behaviour. You have to use a bathroom and kitchen she used. How do you get on with that? Because I know I wouldn’t be able to use the bathroom.’
I replied, ‘It’s less fuss to just wait until she’s been out of the area for enough time. The time factor is to allow for any airborne germs to settle, after which point I just have to avoid touching certain surfaces, which my procedures already account for, not to mention my handwashing and lack of bringing skin biota to any openings in my body. I’m very clear on that.’
At age 20, I stated:
‘In schools and colleges, the airborne disease has been impossible to avoid.’ My friend replied, ‘Yes, which is why I squint and breathe outwards and don’t breathe for as long as possible.’
I replied, ‘Yes. I always had to take breaths in the cleanest areas and go into quarantine mode in the enclosed indoor areas.’ My friend replied, ‘I actually go to a corner to breathe.’ I replied, ‘Yes, me too.’
My friend continued, ‘My mentor was asking what I was doing, because I was walking back with her to leave through the library, and I suddenly darted right and breathed against the wall, in a corner part.’ I replied, ‘Yes; I do that.’
My friend continued, ‘But I’ll try to hold my breath for as long as possible.’ I replied, ‘Did that too, but it’s impossible when you’re stuck in a classroom, forced to conform. I’m certain that’s where the disease-spreading occurred, less so in the hallways and corridors, because of my measures.’
At age 20, regarding a meeting for those with Asperger syndrome, I stated:
‘Yes, they had their teas and coffees and biscuits; that was all there.’ My friend replied, ‘Yes, but why? Why would anyone drink out of a public cup, and why would anyone eat out of public biscuits?’
I replied, ‘Exactly what I was thinking. They mentioned an attendee who usually eats all their biscuits. I was offered by the host, instantly refused.
I was also offered a seat numerous times, refused all times. I remained standing, the whole time, in the exact same posture, looking in the exact same direction, for nearly half an hour, until my dad had to leave due to parking restrictions, and I came with him.’
My friend replied, ‘Yes, but you realise that the biscuits would have been touched when someone goes to take out a biscuit. It is quite common to pick up 2 accidentally and put the other back or to come into contact with the lower one.’
I replied, ‘I’d already established that years ago, which is why I never pick from communal food ever.’ My friend replied, ‘So it surprises me how someone could do it, yes.’
At age 19, my friend stated:
‘When I’m in public, I’m fucked, especially when using a public keyboard. I’m not used to being that restricted, so I end up having a hard time, itching with the back of my wrist.
I itch my head and face with the top of my wrist, and not the one that touches the table. I wash my whole arms when finished and wash my hands 5 times. I usually wear a jumper, though, to prevent having to wash my arms.
Even now, when I’ve used a public microwave, I’ve put my plate on an A4 sheet of paper in front of my keyboard, because someone could be ill and put their plate in the microwave, touching the bottom of the plate, which could have transferred to my plate, so if I don’t put it on a piece of paper, when the plate is gone from in front of my keyboard, it will then be on my wrists, and so on.
I have never sat down to use this computer without washing my hands, never, so this keyboard is very clean. I also used a Dettol wipe on the mouse and keyboard. I eat at my computer, and I touch my face at the computer, so that is my final wall of defence, washing my hands, and it allows me to have the freedom at the computer to itch and pick what I want.’
I replied, ‘I use the lesser used fingers: 4th and 5th usually, as long as it’s not an orifice. As long as it’s purely external, I will scratch.’
At age 19, my friend stated:
‘I have a difficult time with [plates], because I know they haven’t been washed like I wash mine at university, so I’m constantly feeling sick, especially when I get a whiff of dog.
I get stuck then, because the plate has been selected and food dished out, and we are sitting at the table, and then I get the whiff. There is nothing I can do other than force it down quickly, because I can’t complain.
I have my own cutlery. I have a special fork and spoon that is only used by me round my nan’s.’
At age 20, I stated:
‘My mum would carelessly lunge her hands over whatever space I’m using and contaminate my plate below with the hairs and fluff that fall off of sleeves. I had it happen several times several years ago, and since then, I’ve had to make a point of forbidding any sleeves hanging over plates I’ll eat off of, or cups.
I used to see my mum move her sleeve over my plate and then see a fibre/dirt on the plate, having fallen from it. Ever since then, I never hold my arm over my plates or cups. I’ve had my own hair or eyelashes fall into my food. That stops me eating it. It objectively carries the same old contamination risk. My logic is objective here.
It’s not in my hands whether or not my skin or hair has as much bacteria and viruses as others. It would be nice if it were, but it will always catch them from the air, touch surfaces, headphones, t-shirts, pillows.
I still find it a miracle that I didn’t once contract a stomach bug throughout secondary school. It was just about the worst environment for that. Living my life is complex, and yet people have the audacity to say other people live lives as complex as your own.
My gastric infection rate seems totally protected against other people at this rate. My procedures have so far been foolproof against it, even when my family has had numerous gastric infections in the past 9 years, most recently my mum in January 2018, and my sister’s friends have vomited here.
Anyway, the aim is being fulfilled, so I won’t be changing any of my gastric-related procedures.’ My friend replied, ‘Meanwhile, trying to explain to [your mum].’ I replied, ‘Exactly.’
I later stated, ‘I can’t stand people leering over my plates or food or cups or shouting in the direction of them, swiping their sleeves over my plates. It’s all banned for me.’
At age 20, I stated:
‘I was in the kitchen, and I had the idea to verbally exclaim every time I did something that could be considered OCD; it was practically every 5 seconds, like turning on the tap for a split second before washing my glass out with it, to get rid of any sediments around the tap exhaust, or opening the fridge from right at the top of the handle, above my head, to avoid the germs from the area used by the rest of the family.
I also counted many routines of convenience that might not be considered OCD but were still clearly odd and not done by anyone practically, more of those than actual OCD ones.’ My friend replied, ‘Yes, well I do that. I always leave taps running, because dirty water builds up in the pipes, and it is warmer.’ I replied, ‘Yes, that too.’
My friend continued, ‘I open [the fridge] right at the top, while everyone opens it at the side. I open it using the top edge, or my shirt, or my foot.’ I replied, ‘Yes. Good that you miraculously have most of the procedures identical to mine.’
My friend continued, ‘Foot is generally the best one there. Hand at the top is worse.’ I replied, ‘My fridge-handle gap isn’t big enough for a foot.’ My friend continued, ‘Shirt is the worst one in that case. I only use shirt when there is no way of opening something using a foot or touching it in a place another person hasn’t touched, which is most cases.’
At age 20, I stated:
‘I do a lot of cup-vetting. I must’ve picked out 3 or 4 before I chose that one, which I then washed myself in the sink.
I’ve never been infected the way I do my things with cutlery and crockery, so there’s no problem, no reason to do anything different.’
At age 20, I stated:
‘I don’t understand how people put up with the skin-bearing they do. Time after time, I see photos of people with the shortest shorts just sitting on any old thing: public stools, the ground, whatever. Makes me very uncomfortable to look at.
Sometimes, it’s very obvious they’re sitting in potential animal-faeces residues, like in grass, for example, and then there’s wearing short-sleeved shirts and resting entire arms on a pub counter or restaurant/café table, even just sitting on café seats with short shorts.
It makes me squirm. They’re just going to bring that home right into their bed and fester in it, whereas with me, it’s always skin covered, dedicated outdoor clothing, which gets put in a specific area when finished and never has to go near my bed or areas I use regularly.’
I later stated at age 21, ‘I cannot for the life of me understand people who can just brush and knock and scrape and rub their bodies everywhere and on every surface. When I see a girl sitting on a public bench in just a skirt with bare thighs, I cringe to high heaven, same with when I see someone leaning on restaurant tables.
All of it makes me absolutely writhe. I hate how people just plant their hands on the outdoors floor or, worst of all, hold their shoes from the bottom. Drives me insane.’
My friend replied, ‘This all sounds like stuff I saw in primary school.’ I replied, ‘Exactly; I did. The last time I was doing anything like that stuff was when I was in primary school. It stopped as soon as I left, i.e. age 10. There’s no excuse past that age, especially in late teens onwards. You’d expect them to have learnt.‘
At age 20, my friend stated:
‘When I get ill, I track back, list the most likely times of contraction and then eliminate them from my life, don’t do them again. I learn. Nobody fucking else does. They do the same dirty things time and time again.
For instance, I’m never sitting in a public chair again, should never have sat in that chair in the psychologist room. I’ll stand next time. I’m eliminating everything, and if I still get ill, I’m going to stop touching my face altogether, despite the hand-cleaning, and if I still get ill, I’m wearing a mask.’
At age 20, I stated, ‘I keep reprimanding my parents for putting my folded clean clothes on the dirty floor steps, but they keep doing it. I insist they don’t even move them.’
At age 21, I stated, ‘Just realised another “OCD” thing I do; when I rinse out cups, I tip them at the angle such that the water pouring out doesn’t pour out the side I drink from. Didn’t even realise it was weird until now.’
At age 21, I stated, ‘I don’t know what an “OCD-inducing situation” is for me, because it’s non-stop, but obviously, I only have to think of it when I’m put out of control, so not when I’m doing stuff on my computer in my room and my food isn’t falling off the plate.’
At age 21, I stated, ‘Absolutely disgusting: she grabbed [the cup] by the rim, dipping her fingers way in. [For me,] cups are always pulled out with the handle or anywhere on the bottom half. I never touch the parts I’ll sip from.’
At age 20, in response to a YouTube video about ‘obsessive compulsive cleaners’, my friend stated:
‘It’s funny, because they’re touching light switches with bare hands. I haven’t done that in years. They’re all doing unacceptable things for me.
I guarantee I am far more “OCD” than they are when it comes to what I touch. They seem to only be compulsive about what they clean rather than what they touch, which I don’t care about, because it’s not touching me. I don’t care how dirty something is as long as it isn’t touching me.
Me not touching it is clearly better than them cleaning and touching it, for obvious reasons, so I know I’d get ill less. They’d be touching things in public I wouldn’t tolerate, and it’s fucking annoying.
I see that form of “hygiene” OCD about as often as I see the social-mindset form of “eating disorders”. I rarely see my form of hygiene OCD or my form of eating disorder. They’re always caring about stupid things like dust, which doesn’t bother me at all. I’d chose a dusty house over a dustless house with a stinking dog in it.
Again, you see him cleaning the lift buttons, implying he uses it with his fingers. I’m so much more efficient and so much more protected. They’re taking a risk. The wipe they’re using might not kill as much bacteria as they think, but for me, it is 100% every time.
She touched the knocker with her hand. She shook her hand. Come on. It’s the fake-hygiene OCD again, the social-mindset-hygiene OCD, just like the social-mindset eating disorders.
Hahaha, and then he introduced it to his pocket. He shook her hand and transferred it to his pocket, fucking clowns. So now, washing his hands will do fuck all, because it’s now eternally in his pocket.
Also, a lot of the cleaning is based on social impression, the social impression of their house looking “clean” and not “embarrassing” to visitors, the social shame of being “lazy”, whereas to me, that woman’s house wouldn’t bother me at all if it were mine and lacked an animal.
The woman only got upset for social reasons. The man asked how she can bear looking at it, which is a social reason, whereas it wouldn’t bother me. It would have to bother me practically. It would have to present a practical obstruction.’
At age 20, in response to a YouTube video interviewing a person with OCD, I stated:
‘Get out of here. He does not have OCD.’ My friend replied, ‘Probably has the mental-disability version of OCD.’
I continued, ‘Why is he saying he’d pick things up with tissues or socks and wash his hands often? He has tattoos on his digits. He clearly doesn’t care about contamination or polluting his embodiment.’ My friend replied, ‘The hands look dirty with tattoos.’
I continued, ‘He mentioned only recently being able to shake hands with people, and then he touched his hand to his mouth. What is up with these people?’
At age 20, in response to a YouTube comment stating, ‘That’s the worst part of OCD. You know [it’s] irrational yet you still do it’, which had 117 likes, I stated:
‘That’s what really threw me off about reading the OCD symptoms/criteria. It all described irrational compulsions. That’s why I thought it didn’t apply to me when I first read about it at age 14.
I thought I didn’t meet the diagnosis, that it was explained by all my other conditions, which contained the reasons for doing the compulsions I did, the rational reasons, like having routines and procedures due to autism, rooted in practicality.’
I later stated, ‘I need to make a point about OCD not being separate to our condition in our case. It makes total sense, given how both we and [the third person with our lack of the social mindset] have it, in combination with the lack of the social mindset. I think it’s a necessity.
But yes, OCD can come about in other people with the social mindset, like that [man with tattoos] and [another man who had a restrictive-food-intake disorder but was fat], however it will be illogical and not as pervasive.
Ours is mandatory when lacking the social mindset. That’s what I’m seeing, so that needs to be established.’ My friend replied, ‘Higher- and lower-layer OCD again, OCD due to logical thoughts compared to OCD due to a mental illness.’
I later stated in a voice message at age 21, ‘Basically, the lack of the social mindset means that you value and emphasise all the non-social aspects of life way, way higher, so anything that is practically based, physically based, having physical implications regardless of a social bond or anything like that: those get heightened.
Things like germs: when we see an interaction with someone, the germ aspect gets raised much, much higher, because we’re not thinking about the overall purpose of the interaction. We’re thinking about just the physical stuff we’d get out of it, the physical implications we’d get out of it. Germs becomes one of them, and that becomes a high aspect.
And so, I’d emphasise, as a person with a lack of the social mindset, the fact that I’m not passing on germs to people that I am not interacting with.
To them, that’s nothing, because they have that burning, burning desire, that core desire, for the bond, so that overrides and overrules and just completely obscures the actual, physical, real benefits.
You know, that’s a real benefit, to not have germs and not have infections and all that stuff, but to them, it’s so small, because they’d rather socialise, of course, so it looks like I’m doing something wrong when I’m not doing that, even though I’m actually giving them a practical benefit.’
I had previously stated, ‘Our OCD is greatly heightened because we lack the social-mindset funnel that’s allowing it an extra chance at being pulled out, hence why that OCD tattooed, hair-dyed man with BPD [borderline personality disorder] said his OCD was cured when his therapist told him it was a lie he built for himself after his abuse. That’s why that worked on him, and [our neurology] therefore makes our OCD worse.
All of our time is spent accruing knowledge. Practically no time is spent socialising or considering a social role, what I could do for someone else, what I could be for someone else. It’s just constant knowledge.‘
I later stated, ‘For the social-mindset person, social influences are feeding into that learnt fear. Foreign thoughts are becoming theirs, whereas for us, it’s only empirical, observable knowledge.’
I later stated, ‘Autists of the Middle Ages couldn’t have been germophobic, because they couldn’t have known about germs. People like me are a product of being put in the time we were put in, mass-absorbing the information of the time without regard to social phenomena.’
Need for order
A need for order has been described in OCD[8] but also in autism spectrum disorder (ASD).[9]
We would likely be considered to have this feature.
As a child, both of us had the typical ASD behaviour[9] of lining up toys or stacking household items.
In childhood, my friend displayed examples that he later recounted at age 19:
‘I’d stack stationery in class and at dinner. I stacked up glue sticks and stationery on the table. Basically the whole lesson was spent me playing with stationery.’
I replied, ‘I lined up every single toy in the house down the hallways and down the stairs and would build towers out of objects in school. Yes, glue sticks.’
At age 19, I stated:
‘I have possibly the longest attention span ever. I always get that from people about my activities. They always wonder why I stay at something for so long or do something in such detail. They don’t know how I can do it.
I’m the kind of person who would manually scan 100+ PC folders with my eyes for one file if I had to, who would delete or download or copy hundreds of files one-by-one if I had to.
When I do start a repetitive task like that, I make up strict rules in my head so that the repeats stay as the-same as possible. I make up standards, like my mental/food diary: every sentence is constructed in the same way. It’s a syntax of building blocks, a programming language almost, not prose: “At <time> I had <food> [and <food>] [with <drink>].” That’s it, no comma either, been like that for 3 years.
It makes it easy to read, because it makes it easy to spot the differences, to spot where I had a really bad day with lots of text, because I can ignore everything that’s the same and just find what’s different. It’s a classically Aspergic mind.’
At age 19, my friend stated:
‘I was about to take a tablet, and my nan had got the yoghurt and knife out and put them next to the tablets. I took out a tablet, and then I went to the fridge to get a yoghurt and a knife from the drawer. Both times, she said, “There’s already one there.” This is why you don’t interfere, because I’ll still do the procedure.
It’s like how my nan told me countless times the cream is in the kitchen, and when I went to look, I went in my bedroom and couldn’t find it. My bedroom is where I last put it. I do it every time whenever someone moves something or does half of what you do. It ends up not helping in any way, ends up wasting more of my time.‘
At age 21, I stated:
‘I was going to say, I think the “restricted, repetitive interests” of autism are due to less social-mindset replacement, but I questioned it due to how many autists have a significant social mindset. It’s a point to consider and investigate later, but it’s not just interests, is it? It’s OCD behaviours, restricted behaviours.
I’ve done what you’re doing now, putting food in the same place on the plate, but it’s for a practical reason, like absolutely everything else I do.
It’s because it’s an arrangement that gives space for my fork in the easiest-access place [the top-right of the plate], gives space for ketchup and allows for access to the food that needs cutting with the fork.
I do it because it’s the best, most practical arrangement, and so there’s no point doing something different. I came to it gradually, through trial and error, from previous, worse arrangements, so why go back?
It’s restricted in their eyes. What I do in my daily routines I don’t feel is restricted, don’t feel any restriction whatsoever. There are many many ways they could be better, but I’d have to own my own house, and because of lacking the social mindset, I can’t do that yet.’
Hoarding
Hoarding has been reported as an OCD-related behaviour.[10]
We would both likely be considered to have this behaviour, however, like our other OCD-like behaviours, we do not consider it a source of distress nor the associated thoughts unwanted.
At age 16, I stated, ‘I hoard in real life and on all my electronic devices.’
At age 18, I stated, ‘Exactly what I do, photo hoarding.’
At age 18, I stated, ‘It’s why I hoard both objects and digital data. I save for a rainy day. I have that mentality; better to have it and not need it that to need it and not have it.’
At age 20, my friend stated:
‘I only hoard physical possessions because there isn’t an impetus to throw them away, and there might be a time where I will need it. The disadvantages of throwing it away outweigh the advantages. [I also hoard files,] but only because of the same reason. It might be useful in the future, but also, it’s too much effort to throw away.
I don’t delete anything; it just piles up. I only delete when I have to, when I run out of space. I have mass-deleted before and then realised I deleted some things that I needed, but that’s how it works.
I never delete anything until I’m forced, because it’s extra work and doesn’t need to be done. My Downloads, Documents and Desktop folder have about 10,000 items in each.
I haven’t even uninstalled programs I no longer need on my phone or computer or photos I don’t need. Even when I install multiple programs to find the right one, I often don’t uninstall the ones I just installed before it.’
Features we do not have
Checking
Compulsions to repeatedly check locks or ovens are commonly reported in OCD.[10] Neither of us have this.
At age 21, I stated, ‘I’ve basically never had to check any lock, never had to check ovens. I just put it on once and go.’
A 2015 meta-analysis found that those with OCD with germ avoidance procedures performed better than those with repetitive checking behaviours on most cognitive tests.[11]
Compulsions to repeatedly flick switches are reported as a common OCD behaviour.[10] Neither of us have this either. Instead, we both try to touch switches the least, because of germs. I use my knuckle to touch switches, especially that of my little finger, while my friend uses his elbow.
Forbidden thoughts
Forbidden thoughts are described as intrusive thoughts of a violent or sexual nature, such as worries that one may commit a harmful or immoral act.[7] There are also mentions of religious or superstitious intrusive thoughts or compulsions in OCD.[12] Neither of us have this.
At age 21, I stated:
‘I find it silly, actually, when I see people going on about the OCD where they get thoughts of paedophilia or killing a family member, and they say it torments them, and they are endlessly struggling with it and in torture and wish it would stop. I find it so silly. Get over it. What does it matter?’
My friend replied, ‘Is that real?’ I replied, ‘Yes: search up paedophilia OCD or whatever its name is. Yes, that’s the nickname they call it, “Pure-O”, to console themselves. Reminds me of “Aspie”, hate it. You don’t need to be consoled. What the hell is so scary about a thought about paedophilia?’
I continued, ‘I can’t even say whether I get those things, because even if I do, they cause me no distress. I can’t imagine being distressed out of OCD. In fact, it is a lack of OCD that would cause me distress.
Every thought I do has a reason. Even if it is something like what you said [about going back 100 tabs for seemingly no reason], I will have a reason for it that I will be able to justify in the time. I simply never operate without reason.’
At age 21, I stated:
‘I’m sick of people with OCD behaviours going on about them as if they’re bad, debilitating or something they wish they didn’t have.
It is that fact alone that made me believe I didn’t fucking have the disorder, because it wasn’t causing me distress to have the behaviours, of course, the opposite, would cause me distress not to have them. I feel perfectly fine with them. Things are going fine.’
My friend replied, ‘It’s a different condition, what they have.’ I replied, ‘It’s a deformed, twisted, social-mindset version. I presume that’s really just what happens when you put the social mindset into a disorder that is causing no harm or less harm than if it weren’t there.’
My friend replied, ‘It does seem to exist, and the people I’ve seen with it do do those things.’ I replied, ‘Yes. I know it exists, and I know I have “OCD”, because of neurological research, not to mention my tic disorder.’
I continued, ‘None of my “compulsions” are illogical. I don’t consider them compulsions, anyway. I don’t feel anything. They’re just natural ways of doing things, as per logic, how I’d naturally do things if you let me choose the best path, given my knowledge.’
My friend replied, ‘OCD, when referring to us, seems to be a dressed-up way to describe logical behaviour.’ I replied, ‘Exactly.’ My friend continued, ‘It’s people who don’t do those things that I can’t fathom.’
My friend continued, ‘It doesn’t make sense. Why wouldn’t someone need to have to research to that degree and need that degree of control? How can they just ignore those details and have gaps in their knowledge?’
I replied, ‘I have to really dig deep to think of anything I do that could be considered OCD, let alone their type of OCD, because I don’t feel or recognise it. All of my behaviours are just natural to me.
Like [the way things are placed on a table], for example: obviously, all things in my room stay where they are, and I wouldn’t like them moved, because I’d lose track, but no one comes in my room, so it’s never an issue.
There’s no reason for a lot of things to be moved, none at all, just creates confusion. When there’s no net gain, why do it? There’s only a net loss. That’s it; I’m googling common OCD behaviours. All this checking nonsense, never had to do.’
I then sent a screenshot of common OCD behaviours that included ‘Excessive double-checking of things, such as locks, appliances, and switches; repeatedly checking in on loved ones to make sure they’re safe; counting, tapping, repeating certain words, or doing other senseless things to reduce anxiety; and spending a lot of time washing or cleaning’.
I remarked, ‘Only the last one. They paint the hand-washing as if it’s a universal OCD thing; wrong. It could not have happened before knowledge of pathogens. It requires knowledge. It’s my knowledge of pathogens and lack of social mindset that leads me to wash.’ My friend replied, ‘I bet their hygiene is worse than mine.’
I continued, ‘I don’t know where [the flicking of switches] comes from. Funnily enough, I try to touch switches the least, because they’re dirty.‘
I continued, ‘Paedophilia OCD is also social mindset, any violent-thought OCD, created by the social mindset. “You may try to avoid situations that trigger or worsen your symptoms or self-medicate with alcohol or drugs“; I’m done. Funnily enough, the key-checking one requires that you go out.’
I then sent a screenshot stating a feature of OCD as being ‘Requesting or demanding reassurance from family members or health care providers, such as “Have I molested someone?” or “My hands should be clean now, right?”‘
I remarked, ‘Disgusting, never ever ever. I have to add this to the site, unfortunately, and clarify, didn’t want to have to. I can’t think of anything pointless about my behaviours. Everything has a point to it, more or less.’
I then sent a screenshot stating a feature of OCD as being ‘Fear of losing control of yourself by acting on thoughts or impulses, such as harming someone, stealing, blurting out swear words or becoming violent.’
I remarked, ‘Funnily enough, that manifests in tic disorder, doesn’t it? It’s like that’s when they can no longer control it. I think that’s how I have to frame it as, because clearly, stupid people can get OCD and do stupid behaviours.
I even saw worries about God, so I have to frame [the “OCD”] as being a side effect of our condition, or basically, it’s modified by our condition.’
At age 21, I stated:
‘Once again, I can’t think of any way I arrived at my procedures other than a logical one, as in, I can talk through the reasons as to why.
The goal [infection avoidance] essentially remains the same. I’ve sometimes realised I had a behaviour that went against the goal, then I had to assess whether the risk was worthwhile maintaining the behaviour.
Usually, it has been, if things are going fine as they are. I’ll tell you what wasn’t going fine: getting infected by my family and losing kilos at a time, so that absolutely has to be defended against.
Obviously, you know the alarm bells I was talking about [when my friend mentioned being unable to identify a logical reason behind a select few of his behaviours]; obviously, the social mindset is at play. It falls in line with the stuff I’ve read about OCD online, where it can encompass very social-mindsetted concepts or behaviours.
The funny thing about the social mindset is that it’s some spectre that’s constantly trying to hide from us, and we have to poke it out.’
At age 21, I asked my friend:
‘Do you have OCD fears about committing harmful acts?’ My friend replied, ‘What do you mean?’ I replied, ‘Exactly. Apparently, it’s a commonly reported OCD feature, but I don’t consider myself to have it.’
I continued, ‘You mentioned something similar before [imagining “committing an outrageous act”, having to “fight the urge”, “[not] liking it when it happens” and feeling like he “could lose control”]. That’s why I’m asking.’
My friend replied, ‘No. It doesn’t make sense. How can I fear what I’m going to do when I have control over it? How would I have a counter-emotion? I would have accepted the consequences.’
At age 21, I stated, finally explaining why our thoughts and behaviours are not ‘unwanted’ and why the clinical definition of OCD involves such distress:
‘This has stuck in my head while editing our OCD section. Basically, every facet of your OCD has been slightly infected your greater social mindset more so than mine.
It is literally the only reason why those with OCD consider their behaviours irrational and also the only reason why they are in fact irrational.‘ My friend replied, ‘Well, I’ve just got more control over them than them.’
I continued, ‘But it sheds light and is important. It’s an important light on the pathophysiology of OCD.
Obviously, despite its clinical definition literally relying on the social mindset to exist that way, most people with the social mindset do not have OCD. Whilst you need the social mindset to have it that way, having the social mindset doesn’t always lead to it.
But lacking the social mindset like we do always leads to “rational OCD”, which ends up being almost neurologically equivalent to clinical OCD: also involving hyperactivity of the ACC [anterior cingulate cortex]; also having comorbidity with tic disorder.
The only difference is the lack of the social mindset. It doesn’t infect the reasoning centre of the brain [the medial prefrontal cortex and ACC].
What it means is that OCD isn’t something inherent to the social mindset, but it is catastrophically affected by it when it does occur, so much so that the diagnosticians literally don’t know any other way it can present. The only way it’s known to present is with illogical, unwanted behaviours, but it doesn’t have to.’
My friend replied, ‘This appears to be correct. Yes, there was an original mechanism; now, their OCD behaviours are just the OCD mechanism working with the adoption of those specific behaviours, those same old ones that you see on TV. I can produce a [TV-series] video that shows how it’s portrayed constantly. It’s an exact reflection of what real people face as well.’
I continued, ‘It’s because it involves the very regions of the social mindset, the ACC. That’s why the situation ends up like that.
Basically, it seems that all OCD is is hyperactivity of the dorsal ACC, more activity there before it is output into action, but for those with the social mindset, a lot of crazy shit happens: a) appropriated thoughts can form part of that activity; b) thinking of the thoughts can itself regulate behaviour, let alone the thoughts regulating innate behaviour.
So that’s where the clash arises, the conflict, the “unwantedness”. They are thinking of thoughts that, in their case, have been attached to brainstem responses [which triggers the attached responses], but because they are thinking about them for longer, ruminating, due to hyperactivity of the dorsal ACC, it causes considerable conflict with their innate survival mechanisms [which trigger other brainstem responses in their own ways].
I just don’t have that, because I don’t have appropriated thoughts [and their attached brainstem responses] conflicting with my innate survival mechanisms, no second reference for conflict to arise, no source of conflict, no meaningful brainstem infection of my medial prefrontal cortex.
I don’t have a drive to just sit there and think about OCD thoughts. It only occurs when I’m faced with a threat to survival. It’s part of the system regulating my innate behaviour. It hasn’t been infected with brainstem signals.
It doesn’t conflict with anything. I just happen to have hyperactivity of the ACC. I’m just thinking more before doing. I’m considering consequences way more than other people. That’s it, really, almost certainly due to more brain matter elsewhere and less matter [in the ACC].’
I later stated, ‘I will get this clear: obviously, although germ avoidance presents in regular, social-mindset OCD, it’s a non-social-mindset worry. It’s avoiding a threat to survival. However, the reason it presents in social-mindset OCD is because more ACC activity will do that regardless, ruminate over all memories, not just social-mindset-linked ones.
However, [the OCD] becomes deformed when you have the social mindset, infected with social-mindset memories, like you described about those people cleaning and making things look good for others.’
Motor
Both of us have motor symptoms that also appear to be related primarily to the hyperactivity in the dorsal anterior cingulate cortex and its connections to the motor cortices.[13]
Fine motor
Both of us have the fine motor clumsiness that is characteristic of autism spectrum disorder (though a 1998 study found it to be less severe in Asperger syndrome[14]).
My handwriting has always been poor, and it has hardly changed since around the age of 7. It has always been impossible for me to fully stay on the line or keep all letters the same height and in a straight line. The writing also has a relative lack of curves and has more jagged edges. I can write neatly, but it takes significantly longer than my natural speed. My friend’s handwriting is clearer than mine.
Despite having learnt to play the piano, I was often not able to accurately hit certain distant notes. I do not have this difficulty when it comes to typing, because all keys are within a short range.
This feature also affects my facial movements and coordination in a subtle way, such as the lateral movement of my jaw whilst speaking (which does not affect the speech).
Swallowing difficulties
Both of us have swallowing difficulties.
These include:
- being unable to swallow tablets
- being unable or it being very difficult to swallow certain foods
- always needing a drink with food.
These are elaborated below.
At age 15, my friend stated:
‘I’m still eating. I eat slowly. Baked beans take me 1 hour to eat.’ I replied, ‘I hate baked beans, because they take ages to eat. They’re so hard and fibrous that I take ages to chew them, like 2 whole minutes to chew one bean.’
My friend replied, ‘Yes. Hahahah, I’ve been eating this bowl of beans for 1 hour and 20 minutes.’
At age 17, my friend stated:
‘I have a phobia of taking tablets. It always causes an argument, because I cannot take them, and I get called ridiculous, because I keep spitting it out again. I can’t take them. My oesophagus closes up.
I think that I’ll choke. I think that it will go into my lung, because I’m swallowing at a time that isn’t at the dinner table. It feels wrong.
I can usually take the first couple of tablets, but then my mind gets the better of me. I hate it. I’d rather be in more pain than ease it and have to go through that ordeal.’
At age 19, I stated:
‘I’ve had problems the past days. I’ve probably gone into the 46 kg. It’s not good.’ My friend replied, ‘Because of the eating issue?’ I replied, ‘Yes. It’s been particularly bad the past days.’
My friend replied, ‘There was one day, about 6 years ago, I just couldn’t swallow. I thought too much about it, and I physically couldn’t swallow, so I was unable to eat. I don’t know how I got out of it, but it lasted a week. It was a mental fear that I would choke or something.’
I replied, ‘I haven’t had exactly that, but I have a lot of problems swallowing some foods.’
At age 18, my friend stated:
‘I’m often hacking some food up or gripping the table dramatically in order to swallow. I also eat very slowly. I feel like I can’t swallow sometimes or I’m going to choke, and it makes me lurch and grip onto the table.’
I replied, ‘I have a swallowing problem. I always wince when I swallow, and I need to drink with it usually.’
At age 19, in response to my friend describing his swallowing difficulties as mental/fear-related, I stated, ‘I have trouble swallowing, can’t eat without drinking, as you know. It’s not something I have to think about. I just have trouble swallowing.’
At age 19, I stated:
‘I have to have a drink with everything I eat, otherwise I risk choking.’ My friend replied, ‘Same.’ I continued, ‘I have to put the drink in the mouth with the food and swallow, because saliva doesn’t suffice.’
My friend replied, ‘Actually, I ate a McDonald’s in the car once, and I didn’t have a drink, and I was suddenly overcome with fear, because my mouth went dry, and I felt like I was going to die, with no access to water.’
I replied, ‘Yes. That’s happened to me with crisps.’ My friend continued, ‘In general, I always misswallow things and have to hack them back up and swallow properly.’
I replied, ‘If I go anywhere that I think I’ll need to eat while out, I bring a bottle of water, obviously bringing my own food too like crisps. I meant eating my own food while out, due to the duration.’
My friend replied, ‘Everyone I see eats dinner without a drink, my nan and grandad, but I have to have a drink.’ I replied, ‘Wtf? I haven’t actually seen that. I can’t imagine eating anything without a drink.’ My friend replied, ‘Same.’
I continued, ‘With chocolates or biscuits, it’s always milk. With savoury foods, it’s always Pepsi. With anything I have to take outdoors, it’s water.’
At age 20, I stated:
‘I stopped eating sandwiches at the start of secondary school, because the bread soaks up all my saliva. I have an issue with dry foods that soak up my saliva. I can’t eat them, except extremely laboriously and time-consumingly: baked beans, sweet corn, rice, couscous.’
My friend replied, ‘I can’t eat without a drink, because my mouth goes dry, and I panic. I can’t swallow, and I sit there for ages with a mouthful.’
I replied, ‘Exactly. I get exactly that. Even with a drink, it’s hard, but without, it’s impossible. I avoid, because it’s too bothersome. There are easier foods out there that I’ll finish the plate of and put on weight from. No point choosing a laborious food, none at all.’
At age 20, I stated:
‘I eat alone all the time now. I would feel uncomfortable eating in front of other people for a multitude of other reasons.
Essentially nothing can go wrong as long as I have a drink on hand, which I always do. I practically can’t eat anything now without a drink. I’m finding that I will be guaranteed to choke if I eat crisps without a drink now.
I’ve been a slow eater all my life. I’ve seen it, how people eat 5–10x faster than me. I don’t know how it’s possible, but it is. I’ve had to be faced with it all my life, sometimes as a cause for embarrassment.
Every restaurant I ever went to, everyone would finish more than twice as fast as me, and they’d get fed up of me still eating, so I’d have to hand in a half-full plate.’
At age 19, my friend stated:
‘Do you ever clench your fist when swallowing, or grip onto the desk, or push your fork or spoon hard into the plate? I do.
My arm sometimes moves out to grip something. I can’t eat when walking along. I have to stop and hold on to something, but then it looks strange, so I can’t swallow, because I know people are looking at me.
I often take multiple seconds before swallowing. I just sit there on the brink of swallowing, and then my arm goes out, or I grip on the desk.’
At age 20, I stated:
‘Every time I tried to eat roast sausages, I’d struggle. Once again, 6/7 times, the taste of the brand would be off, but every single time, the skin would be inedible, and not only that; the taste and juice would be sucked out of the meat after chewing, and it would make it almost impossible to swallow.
It became like swallowing some kind of soggy dust. It had no taste, but it was a difficult texture to get down. That happens with beef as well. Doesn’t happen with chicken [though it did here].
One reason I’ve abandoned pasta bolognese is because of how much less I eat of it and how much slower. It’s a calculated, tactical move to get as much food into me as possible and as many calories, given the constraints of the situation. I used to have cod fish fingers, but it was always meh, so I couldn’t turn back to it given what I eat now.
I hate discussing food tastes, because I hardly like anything. There’s what I eat, and there’s what I can eat. What I eat has been determined by two things: the constraints of the house situation/my physiology and my own tactical choices to get as many calories into me as I can.
It’s lucky I can tolerate most chicken nugget brands, but not all. It’s part of why I’ve settled on them being my main meal. It’s hard for it to go wrong for my parents when they go shopping.
Everything is calculated. I abandoned many, many foods simply because the frequency of me tolerating the brand or instance was too low. It’s not worth it. I leave most of the plate, and it goes to waste in those instances.’
At age 19, I stated:
‘My nan just demonstrated how she swallows tablets, and it became evident why I’m unable to. She does it with a drink, but I now know why that has never worked for me. She doesn’t swallow the drink; she just tips the drink up, and it goes down her throat.’
I replied, ‘Of course she did. She’s fanatical about it. It’s surprising you’re only having this fiasco now. I had it with my parents some 8 years ago, where my mum was trying to demonstrate to me how to swallow tablets.’ My friend replied, ‘But she lets the drink run down her throat. She doesn’t swallow. It’s this gulping that I can’t do.’
I replied, ‘I don’t know how they do it, and it doesn’t matter to me. All that matters is what I can do. There’s no point them showing.’
At age 20, I stated, ‘I just tried swallowing a chunk of crushed up tablet to see if I could, and it got stuck. It took a second swallow to displace it from its stuck position.’
At age 19, my friend stated:
‘Other people eat a lot faster than me. They seem to be able to swallow quicker without chewing, for some unknown reason.’ I replied, ‘Yes. I chew for minutes.’
My friend continued, ‘… even though I’m chewing as efficiently and quickly as possible and swallowing at the earliest occasion, so I can only conclude they are able to swallow earlier, when the barrier for me is still up, when I’m not ready.’
I replied, ‘They also put a lot larger bites into their mouths. Everything about the way they eat is different.’
At age 20, my friend stated:
‘How bad is your swallowing? Do you find yourself chewing a mouthful for about 5 minutes and swallowing it piece by piece?’ I replied, ‘Well, it was bad today. It varies from day to day.’ My friend replied, ‘Same. Exactly.’ I replied, ‘I had exactly that today.’
My friend continued, ‘I don’t know what’s going on, but I’m not making this shit up. I don’t think doctors would have encountered this issue before, but there’s literally nothing that can make it go away.
For instance, I put one small boiled carrot in my mouth, and I was chewing it for 5 minutes, a mouthful of carrot and saliva, and I swallowed down a tiny portion of saliva at a time, but it’s like my mouth kept filling up with saliva, so it just took longer and longer, but it only happens with certain foods. It happens with meat, potatoes and vegetables, but I chew so much that my jaw hurts, because it’s like I’ve eaten 50 meals in the time.’
I replied, ‘I have multiple different swallowing issues that are different from each other. The issue I had today applied to all foods. There’s the overarching gas/nausea issue I have that prevents swallowing globally, then there are the food-specific issues, like being unable to eat dry food without a drink due to choking, or being unable to chew mince meat for too long due to it becoming inedible, or being unable (or it being very difficult) to eat rice or sweetcorn flat-out.
Today, I had issue 1, which on one occasion led to issue 3. It led to me chewing a chicken nugget for so long that I had to spit it out, couldn’t swallow it. It had turned to tasteless dust. I have a whole array of flavours of gastric issues.’ My friend replied, ‘Exactly. I’ve had that.’
At age 21, I stated:
‘I haven’t been able to eat basically anything without a drink for years; I mean the food and the drink in the mouth together. I have to, otherwise I’d choke or take 10x longer to eat. For example, when eating crisps, the Pepsi supplants the saliva, makes me able to eat it at a normal pace.
I’ve tried eating crisps, for example in school or college, whilst still having a water bottle but not having it primed, and very quickly, I would almost choke and immediately have to whip it out and take a sip a lightning speed, so I always have to have a drink primed, able to be sipped within seconds. Anything less isn’t good enough.’
At age 20, my friend stated, ‘I need a nasogastric tube. I’m sick of eating. If my swallowing deteriorates to what it was when I was 10, then I’ll have to, that time where I was struggling to swallow my own saliva.”
At age 21, I stated:
‘[In addition to your OCD,] your greater social mindset also infected your swallowing difficulties, so that pinpoints the source of those difficulties to the ACC [anterior cingulate cortex], but I’d already stated that’s where they were from, but now there’s confirmatory evidence.’ My friend replied, ‘I really want them to go away. There’s absolutely nothing I can do.’
I continued, ‘It’s because you described them as mental or fear-related in the past, due to fear rather than alongside it; that’s the social mindset. I don’t have that. I don’t have to think about them. They just happen in the moment, just like my other OCD behaviours.’
My friend replied, ‘But they’re scary. Mine are, anyway. Yours are likely different, but every swallow is possibly a misswallow. I want it to go away, because it’s stress, and it also results in less fluid being consumed over 24 hours, because I can’t just gulp it down in one minute like I used to be able to. Now, it’s a gruelling, hour-long process.
I used to be able to gulp water down. Now that I can’t, it’s significantly impacted the amount I drink. Every time I get an urge to drink, instead of that being 500+ ml in one quick go, it’s now 10 ml or less.’
I replied, ‘It’s scary when I almost choke, in that moment, but it’s all in the moment, but obviously, I avoid foods that make me choke.’ My friend replied, ‘For me, it’s when I’m about to make a swallow, but it’s both.’
I replied, ‘I imagine it’s simply because the memories of the fear while choking became social-mindset ones, brainstem-response-attached ones, so you are able to ruminate on them and imagine that fear outside when you are actually choking. You can trigger it again.‘
My friend replied, ‘But whether I’m thinking about it or not, it still happens. I have not been able to make a single swallow above a certain threshold for years, and as soon as I do, it will come to the forefront of my mind.’
Source: [15]. Licence: CC-BY-4.0.
Tic disorder
On Background, I mentioned that both of us had been diagnosed with obsessive–compulsive disorder (OCD), and in the Learnt anxieties/OCD section of this page, I extensively described our OCD-like behaviours.
The comorbidity between OCD and tic disorder (20–60%[16]) is well documented.
At age 20, over the course of a month or two, I developed a motor tic disorder. However, the tics are almost exclusively triggered when swallowing food.
Despite this, unlike the swallowing difficulties that have existed since childhood, the tics themselves do not interfere with my ability to eat or swallow to any degree and as of yet have not caused any level of functional impairment.
In these instances, they do not start until the first mouthful of food is placed in my mouth, and despite them initially coinciding with the swallowing process, they usually repeat for several seconds after each swallow.
As of July 2020, the most prominent tics involved:
- hitting the back of the right hand against the palm of the left hand (which was always followed by the next tic)
- extending the wrist and elbow outward horizontally
- pulling in the right arm vertically against the chest with a clenched fist
- shifting the shoulders and neck
Less prominent tics included:
- widening the eyelids
- deviation of the eyes, typically to the left or upward
- a single deep and rapid inhalation
- clearing the throat
- lifting the left eyebrow (which I cannot do voluntarily)
- scrunching the nose
In mid-2020, the prominent tics involving hand movements garnered the addition of a telephone sign (thumb and 5th finger extended), usually with the right hand or both hands. In late 2020, they garnered the addition of a gesture similar to the OK sign with the left hand but with the thumb and index finger flat and straight.
Despite being uncertain as to whether they were tics in the immediate onset in early 2019, due to the barrage of information emphasising the conflation between stereotypies in autism and tics,[17] it soon became clear that they were tics. They are less severe (or even absent) when I am intently focused on a task whilst eating, such as reading a study, and the severity increases with my general state of excitability at the time of eating. The type of food or drink has not had an effect on the intensity of tics.
Whilst vocal tics have not been a part of the disorder, there have been very rare instances in which, immediately after a severe tic, I said something (usually an expression of frustration) that I was not sure was not a vocal tic (i.e. it felt compelled somewhat beyond my normal compulsion to speak).
At age 20, I stated:
‘The feeling to release a tic feels like it’s always been there but never enough to make it actually happen. It hardly felt any different when the tics came on.
It didn’t feel like the urge that leads them to happen was any different; it just felt like I no longer had control over it. It basically felt no different when they started.’
The dorsal anterior cingulate cortex (ACC) is strongly connected to the premotor and primary motor cortices as part of using knowledge of consequences to plan actions/movements.[13]
In OCD, the dorsal ACC is hyperactive, as described on Neurology of our lack of the social mindset. Tics arise from bursts in this activity during temporary increases in dopaminergic transmission in the basal ganglia motor regions, which re-excite the motor cortices as part of the cortico-basal ganglia-thalamo-cortical loop.[18][19]
I have found no studies documenting a tic disorder centred solely around swallowing food, however it is highly likely that the manifestation of my tic disorder only when swallowing food is related to the disproportionate representation/severity of swallowing difficulties in our motor symptoms, which may or may not be related to the proximity of the swallowing region of the motor cortex to the insular cortex.
The lack of the social mindset likely also has a role in both the low severity of my tic disorder and its exclusive association with swallowing food. It is likely that the dopaminergic cortical excitability threshold for the disorder is only met during combined processes of eating (reward) and swallowing (motor), when the process of eating is one of the few rewards left when the social mindset is almost entirely eliminated and there is substantial inhibition of sexuality, unlike those with social-mindset forms of OCD and tic disorder.
My tics started late compared to most of those with a tic disorder, whose tics typically start in early childhood and decrease into adulthood.[20] It is said that motor tics appear first and that vocal tics typically appear a few years later (around age 11),[21] suggesting they are more intense manifestations of the disorder.
Sensory hypersensitivity
Both of us have significant hypersensitivity of the senses, which alludes to the role of the insular cortex in our condition.
The insula’s role has also been highlighted in regards to disgust, which has either been heightened or diminished with its damage. In our condition, it is heightened. This is likely due to increased excitation of the posterior insula, similar to the hyperactivity of the dorsal anterior cingulate cortex.
This insula-related feature appears to affect sight, smell, touch, taste, pain and temperature in ourselves, however, as mentioned in the Differences between us, I developed an imprinted phobia related to the acoustic startle reflex in early childhood that could be seen as a sound sensitivity, though it is related to the temporal lobe and is not present in my friend.
Sight
Both of us have a sensitivity to bright light and keep our blinds closed at all times. I have also taped the edge of my blind shut with duct tape, since the slit points directly at my bed.
The only light source in my room 24/7 is my computer screen and a single desk lamp, while the only light source in the room of my friend 24/7 is his computer screen and a bathroom light.
Any time I use the kitchen during the daytime and find that the door blinds have been opened, I have to close them.
At age 16, my friend stated, ‘I hate sun, cannot be exposed to sun. I remain in my bedroom. I prefer cloudy.’
At age 17, my friend stated, ‘I am much more sensitive to [the sun] than other people.’
At age 19, I stated, ‘One thing to note is that I absolutely despise sun in the winter months. It’s just about the most sickening thing. I even dislike overcast without rain, because it’s blinding. It makes me feel sick.’
At age 18, my friend stated, ‘I just can’t believe how regular people love the sun. I despise it. It’s ridiculously uncomfortable.’
At age 19, I stated, ‘The sun is directly in my window in the morning, but obviously, my blind is always closed.’
At age 18, my friend stated, ‘The weather forecast makes me angry, how these people can speak so happily, with smiley faces, about “gorgeous sunshine”, “sun beating down”, “Many will welcome these beautiful conditions”. What’s wrong with them?’
At age 20, I stated, ‘I do not like overcast when it’s blinding white, only when it’s dark clouds or rain. When it’s white, it gives me a headache. … The low sun of the winter is also pretty bad.’
Smell
Both of us are extremely sensitive to smell. This is a second reason (in addition to germ avoidance) for why we hold our breath and breathe under our top when entering or passing through certain rooms.
At age 16, my friend stated:
‘There’s a smell I hate: I call it static. It makes me gag. It’s the smell of fleece that’s been in the cold. People have this horrible coat smell, staticky smell.’
My friend later elaborated at age 17, ‘I know it well, because my mum smells of it after being outside in the cold. It’s awful. It’s similar to the cough and throat smell, which I also hate.’
At age 18, I stated, ‘I don’t know why blow-drying my hair always makes me feel sick, and brushing my teeth [with toothpaste]. I get nausea. It seems to be the smells.’
At age 19, I stated:
‘My coke glass smells like old nannies’ cushions, a soft, felty smell of kitsch ornaments on the shelf.’ My friend replied, ‘Hate that smell. That’s a smell of glassware.’ I replied, ‘Oh yes; usually my glasses stink.’
My friend continued, ‘There is another smell of plates where it smells like dog breath sometimes. That makes me sick. If you have a bad dishwasher, the plates can smell like dog.
I’ve refused food in a restaurant before because the plate smelt of it. Also, a spoon did once; my mum agreed and got me another. My mum also goes up and gets me a straw.
It’s the smell of glass coming into contact with substance.’ I replied, ‘It’s definitely the non-brand coke causing [my] smell, gone flat.’
At age 19, I stated:
‘My father’s car: that’s an awful smell. Smells like dust is literally filling my nostrils, clogging them up.
I also know some perfumes that make me feel instantly sick, give me a headache. There’s one my sister puts on every morning, and literally, it immediately seeps out of her room and under my door crack, and I’m woken up by it, an extreme smell, putrid. Any girl who wears perfume will never have anything serious to do with me.’
My friend replied, ‘Just why? I often reel away when I smell a perfume. Yes, same at university. I smell smells creeping under the door, smells of perfume and people, which is why I blocked underneath the door, stuffed it with an old t-shirt.’
I replied, ‘I’ve been thinking of permanent ways to do that with mine, but the cracks are all around the door frame.’
My friend replied, ‘Yes, but think about it: if I can smell that, then it means I’m inhaling whatever else is in the corridor: sneezes, coughs.’ I replied, ‘Yes, exactly. That’s what I think.’
I continued, ‘[I also hate the smell of] some soaps, anything coconut, instant nausea, but it’s definitely not limited to that. Half of all soaps and shower gels and shampoos, I can’t stand.
Unfortunately, I’m subject to the arbitrary rotating selection my mother purchases, but as soon as I’m in control of my own washing liquids, they will remain the same, forever. I will smell them in the shop and make the decision then. Absolutely NO reason to keep changing them. No reason. None. Pointless. What goes through people’s minds? It’s totally bonkers. What leads them to that pattern of thinking?’
My friend replied, ‘That man that was hit and became a savant, woke up a “genius”:[22] as I was saying, he immediately had germophobia, immediately started cleaning in an OCD way, and yet this is a programme showing people someone turning into a genius, but he only has the same practices as us, and yet people just see him as an absolute genius and accept it will never happen to them. People have no idea what they’re missing out on.’
At age 18, my friend stated, ‘I hate random smells. I can smell PVA glue all of a sudden.’ I replied, ‘Good timing, by the way; I’ve just patched up my door cracks with taped tissue for that reason. It’s nowhere near foolproof, but it’ll have to do.’
At age 19, my friend stated, ‘I hate the smell of coffee. Stinks.’ At age 18, I had stated, ‘I do hate the smell of coffee.’
At age 19, I stated, ‘I always hated the smell of garlic bread. It reminded me of cheese, which I also hate. It was just this saltier, more vegetably cheese.’
At age 19, I stated, ‘I’ve never had duck, but when my family have had it, I hated the smell. It ruined my chicken nuggets once. It soaked into them while I was using the oven [while they were also cooking duck], made them inedible.’
At age 18, my friend stated, ‘I hate the smell of new cars. Smells like dead crab.’
At age 19, I stated:
‘[My parents are] becoming so irresponsible with smells in the house that I don’t let them [enter my room]. The kitchen has never stunk so badly. My sister now uses perfume.
I don’t let the door stay open at all for more than 10 seconds. It’s either ajar or closed. I don’t even open it conveniently wide to get in and out; I open it a crack and slip through that crack, because I don’t want the disgusting air blowing in.’
At age 19, I stated, ‘Ffs. Now my room stinks of burnt food. I cannot get away from the smells of the house anymore. I haven’t found anything to stuff my door cracks with yet. Tissues would not suffice. I don’t even think I have enough clothes to use them.’
At age 20, I stated:
‘[My parents] have made it hell to fall asleep in the morning, because of the products they spray all over the place. Also, my mum stormed in, door wide open, when I was trying to sleep yesterday morning, blowing the smells right in. Next time I do end up having to sleep in the morning, I’m locking my door.
I still remember that time a few days ago when I couldn’t sleep for at least 2 hours straight because of the smells they’d sprayed. I literally lay in bed for 2 hours straight, just trying to sleep, doing nothing at all; checked the clock periodically to see how much time was passing.’
My friend replied, ‘Yes. Hair spray, air freshener, perfume: all of them make me cringe and say, “What is that smell?” Pointless. Nobody should want to smell that at all. What’s wrong with them?
These women with pungent perfumes: what are they trying to do? How can they think that smells nice or comfortable? It gives me a headache and remains lingering in my nose, and I can’t smell anything else.’
At age 20, I stated:
‘[When my dad would take me on walks,] I’d hate the horrible smell that sticks in my hair, horrible industrial, plasticky, smoky smell. That made me feel nauseous.
The smell in my hair was atrocious: plastic and rubber and industrial materials and smoke.’
At age 19, my friend stated:
‘You’ll never believe this: the trolley, right, is about 5 metres away from me, and I keep getting this whiff of perfume that smells exactly like my mum, so I walked up to the trolley and sniffed the handle, that I made sure not to touch once during the shop, and, lo and behold, it stank of that smell. I’ve now removed it from my room.’
I replied, ‘I regularly have that situation. I always smell smells a mile away.’ My friend replied, ‘Exactly, in such an inconspicuous place as well. Who else would smell that from over here on such a small surface area?’
I replied, ‘Yes. The thing about my smell is that it’s very quick to detect, very quick indeed. When a smell starts to get created somewhere else in the house, I pick up on it very, very quickly. It’s a jarring change from the ambient smell around me. It hits me like a train.’
At age 20, I stated, ‘There are very pungent smells when I step out my room, a major one being saliva. My parents’ room as of last year has begun to stink of elderly; stinks of dribble.’
At age 20, I stated:
‘The rest of the house stinks: the upstairs hallway in the vicinity of my parents’ bedroom smells of elderly; the bathroom stinks of all sorts of products that my mum or sister have recently used in it; the downstairs stinks of fabric that’s been outdoors; and the kitchen, god, a cocktail of smells, often just flat-out bin smell, because the bin is in a drawer that sometimes gets left open, so it’s a cocktail of rotten food smells.
Luckily, the portholes are easily opened, but unfortunately, they are portholes to the recycling bins, so they themselves let in an air of plastic and paper smell, but at least it’s better than bin. Still, you gag if you breathe it directly from the porthole.’
At age 19, my friend stated:
‘All sorts of disgusting smells, perfumes and cleaning products are wafting under my door. I got in a lift once, and it stank to high heaven.
It was truly the worst smell I’ve ever smelt in my life. It burnt my nose. It made me feel sick, and that was after a single slight inhalation as I entered. I only managed to start inhaling, and immediately stopped, and even those few milliseconds of inhaling, my nose was already burnt out. I immediately coughed it out. It was the worst thing I’ve ever smelt in my life.
It stunk of this old lady cough smell, and then you know what? I saw someone walk out of the lift like nothing had happened. They weren’t even in a hurry to get out.’
I replied, ‘Yes. Our difference in sensation is also due to the neocortical difference, the neocortical enlargement. It’s not a direct low-level nerves issue; it’s a high-level perception/cognition matter. There is more brain activity dealing with the sensation.’
My friend replied, ‘Yes, but surely people can smell that.’ I replied, ‘You’d think so. I think they can, but it’s much less potent. It doesn’t cause an override. The threshold is much lower. We smell things they even don’t smell, and we detect them more instantly.’
At age 20, I stated, ‘I just had a hint of tobacco smell; immediately jumped out of my seat and went to the window, couldn’t see anyone, then I heard a woman’s voice from the next-door garden say “Becca”; immediately knew that’s where it came from. I see these people as no better than poisonous plants or frogs, just things to stay away from at all costs.’
At age 19, my friend stated, ‘It’s funny, because that’s why I don’t wash my clothes at university, exactly why, because I don’t want to put it in the public washing machines, because of the smell, the substances, the dirty water and residues of other people’s clothes, the smells of their washing powders and perfumes, and that’s exactly why I wash my clothes in the bath with my soap.’
At age 21, I stated, ‘Just got reminded of why I don’t cook in a recently used oven again. Decided to be lazy and not leave enough time for a gravy smell to leave before I cooked this time – it’s fully infused in the food. At least it’s not duck.’
At age 21, I stated:
‘My ideal ventilation would be a pipe that sticks way up out of the roof, as far away from neighbours as possible, because I’ve experienced first-hand the torture of neighbour smells wafting through the window, the smell of their house.
More awful smells are coming through the window. Seems like they’re different each time. Just now, it was some disgusting perfumey grass smell, like a strong flower fragrance.
The worst one was this strong, sugary, tickly, meaty one that I distinctly remember was the smell of the neighbour’s house in childhood, most nauseating. I’ve had burning smells come through, cannabis.’
At age 19, my friend stated, ‘Gross: I bought this drink from the shop and stopped dead, because I could smell a tribal smell. Right, washing all bottles in future before drinking.’
At age 19, my friend stated, ‘I know all sorts of smells, and it affects me more than others. There are thousands of smells, but I hate smells. I can smell many and a lot more strongly than other people, who don’t seem to be able to smell anything.’
At age 20, I stated, ‘I got 1 hour of sleep lol, was woken up by an extremely pungent perfume and a lot of nausea.’
Touch
Both of us are sensitive to tactile sensation.
Both of us cannot stand any kind of clothing that features abrasive material, such as jeans or other denim.
My friend cuts the tags off all clothing items he wears. My clothing ensures that no areas of skin are exposed from the neck down except the hands. I am unable to brush my bare palm against a surface, and I am never barefoot except when showering.
At age 15, my friend stated, ‘I’ve never worn a watch. I hate the feel of something around my wrist, on all those tendons and veins. Ugh.’ I replied, ‘I did wear a watch to school for a few days, but I didn’t like the feel too. I’m sensitive in all my senses.‘
At age 17, my friend stated, ‘The feeling of a watch on my wrist makes me feel ill.’
At age 17, my friend stated, ‘The tag on her clothing turns me off greatly, the white thing. It’s making me gag.’
At age 18, my friend stated, ‘The feeling of cold, sticky plastic on the clothes sets my teeth on edge. It kills. It makes me sick. I hate any form of ticket, tag and logo on clothes. They need to be removed.’
At age 18, my friend stated:
‘It’s actually gross. I couldn’t wear makeup as a girl, not even because of who it makes me look like, but because it’s just disgusting. The texture, the feeling of that on my skin, the smell, the presence. How can they put up with that?’
I replied, ‘Yes, well it’s everything, isn’t it? You’re just proving how the list of reasons is thousandfold. I hear about girls who wear minimal makeup saying they don’t like it because it feels heavy.
When I had face paint on as a child, it felt restricting, like there was a spider’s web over my face, pulling it together, holding it in a position.’
At age 18, I stated, ‘All my senses are sensitive, my touch too; I can’t rub my palm on most surfaces. I cringe.’
At age 20, I stated, ‘That YouTube Asperger’s girl was wearing hoop earrings in her latest video.’ My friend replied, ‘She doesn’t have the sensory issues that should prevent that, such as the weight and the constant tugging at the ear lobe and the feeling of cold metal slapping against the cheek. It’s nothing that I would put up with.’
At age 19, my friend stated:
‘You know, what is that fucking glitter these girls have on their faces?’ I replied, ‘Yes, see that a lot.’
I continued, ‘You know girls: it’s like they try and do the exact things they know will piss off autists the most. They put the most ungodly shit on their skin that any autistic sensitivity could never bear.
I end up seeing them as shop-window dummies, because it’s like they don’t feel anything, like they’re just made of wood.’
At age 19, my friend stated, ‘I cannot stand the feeling of sweaty leather against the skin. I hate leather.’
At age 19, I stated:
‘I never walk barefoot. It’s mainly germs and the sensation, like how I was forced to be barefoot in the seconds before I get in the shower. I hated walking in the hair that’s on the ground.
I don’t take my socks off when I sleep [due to rubbing on the duvet], a practice since about 4 or 5 years ago, and I just realised that will get noticed by any girl I’m with, just like how you noticed how I tucked my trousers into my socks so they wouldn’t roll up while I’m asleep.
I forget I do these things, always. It makes me wonder how many ridiculous practices I’m doing that I’m not even aware of. I know a few things, but I don’t know the full extent of it, and these small experiences remind me of that fact.’
At age 19, my friend stated, ‘The clothes people wear are so ridiculously unwieldy. I wouldn’t be able to wear any of the clothes they wear without feeling extremely itchy or uncomfortable, cringing at the feeling and location of the fabric and the sensation and the texture.’
At age 21, I stated, ‘Trying to imagine me wearing something that minimal around the house is hell, because immediately, this is what comes to mind: … all of the scraping and scratching against the back of my chair and arm rests; all of the dead skin and hair it will be brushing up against; all the easy exposure of that skin to the downstairs air and germs of the family.’
At age 21, I stated, during the summer, ‘This happened last year [too]: for some reason, when I open the window, I feel small pricks all over my exposed skin, as if flies are landing on it, but they aren’t, and it feels smaller than flies. Could be humidity; I feel it on my scalp as well.’
Taste
Both of us are highly sensitive to taste, though this is mostly due to the contribution of smell, since the taste buds can only differentiate between a handful of tastes.
Both of us are highly sensitive to differences between brands of the same food, changes in the same brand of a food over time and differences in the location where the same brand of food is bought from (indicating a different manufacturing facility).
At age 15, my friend stated, ‘I hate those sausages that have a really disgusting sharp, plastic taste to them.’
At age 19, my friend stated, ‘I’ve never actually liked popcorn.’ I replied, ‘Nor me. Tried it once, hated it, and hate the smell.’
At age 19, I stated:
‘I had to stop eating those [cookies], because multiple packs kept being bad, having a horrible rotten fruity taste, so now I’ve switched back to Oreos. It’s been a flip-flopping switch since Year 6.
It was a fundamental, out-of-the-packet taste. It was such an issue to me that I contacted the company by email, and they replied, saying they’d forwarded my comments to the quality manager.’
My friend replied, ‘Probably because it wasn’t double chocolate. I imagine the original ones are shittier.’ I replied, ‘I’m referring to the double-chocolate ones. I’ve never had the normal ones. Obviously, I would know, being me, the person with the most sensitive taste and choosiness for brands ever.’
I continued, ‘They introduced a new packaging with a different name, and the original packaging acquired this horrible taste, so I switched over, but as of late, the new packaging acquired the [original packaging’s] taste in some packets, too many for comfort, so I stopped eating them.
The funny thing is, I’ve experienced several different Oreo tastes depending on where and when they’re from, though they generally tend to be good.’ My friend replied, ‘Yes. It depends on the shop for some reason. There are so many factors.’
I replied, ‘All ones from that batch my mother bought had one taste, and now, I’ve been bought another one, and it tastes different; worse, but still edible. It has more of a soily taste, like damp soil.’
At age 20, I stated:
‘I had yet another bad-taste encounter with a same product, Pepsi this time. My dad bought a local 1.5L bottle instead of the normal 3L ones; tastes totally different, much worse but still bearable.
On the other hand, the second half of the Oreo packs my mum bought seem to have the best Oreo taste I’ve ever had in my life, in contrast to the first few of the batch, which tasted slightly plasticky.
I would honestly struggle to believe how people couldn’t taste the differences I’m tasting. I think they can, but they just don’t think about it or care, because they like everything, can eat anything. I can’t.’
My friend replied, ‘Yes. Pepsi tastes like shit in cans. Only McDonald’s or draught coke is nice. It also tastes like shit in bottles. Yes, it is ridiculous.’ I replied, ‘Haven’t had one in a can in forever. The McDonald’s one is very nice, yes.’
At age 19, my friend stated:
‘The situation becomes even more complicated when you move about like I do and eat at university, home and round my nan’s. The food tastes different in all environments, even if it is the same exact spoon, bowl, cereal, milk. If I eat it round my nan’s, it will taste different.
It’s something about the air. The air of the house smells different, and of course, that will be taken into my mouth, and it makes the food taste different, so when you add that complication, it gets even more complicated.’
At age 19, my friend stated:
‘I was a very fussy eater as a child, rejected certain plates and spoons, had to have the same cereal, same bowl, same spoon and eat in the same room.
I find eating in another place changes the taste, and I’m not wrong. Eating my cereal round my nan’s in the same bowl with the same spoon, same milk, same cereal, imported from my mums: it tastes different.’
At age 19, my friend stated, ‘Do you know the most disgusting and pointless fruit? Avocado. I hate how people eat all these exotic foods. It all tastes disgusting, and it’s all unnecessary.’
At age 19, my friend stated:
‘I swear when I buy bottles of Pepsi Max, it tastes like sharp shit, but when they serve up a bottle in a restaurant or KFC, it always tastes nice, same exact bottle.’ I replied, ‘I don’t drink Pepsi Max ever since years ago, when it became awful.’
My friend replied, ‘I only like Pepsi Max draught. All other cokes and Pepsis are generally awful, especially can, bottle and glass.’ I replied, ‘The 500ml does taste worse but still bearable. 2L is best. Cans were ok but, again, not as good.’
My friend replied, ‘They taste different from shop to shop and restaurant to restaurant, despite the same exact bottle; what I mean is from KFC to KFC, because they give you a bottle, a 2L one.’
I replied, ‘Lol, I’ve only eaten at KFC once. I’ve also only eaten at Burger King maybe 1–3 times. And it wasn’t a meal [at KFC], only an Oreo Krushem milkshake, which was disgusting.’
At age 20, I stated:
‘Unheard of for me [to finish my plate] all of the time. It happens between 1 in 5 and 1 in 50 times. It’s impossible for me to imagine easily gaining weight.
I gave up on Sunday roasts ages ago; too unreliable. It would be too different each time. It’s also the reason I’ve given up on bolognese. My mum would make it, and each time, it would have a slightly different taste. Usually no issue, but sometimes, it would be inedible, so I thought, I’m at the brink of starvation; I can’t be dealing with this anymore, so it’s chicken nuggets everyday now.
Before I gave up bolognese, I gave up rice; too difficult to swallow, and before that, sweetcorn for the same reason. I was doing my whole family a favour by giving up certain meals. It meant they didn’t have to waste money on them just for me not to eat them.’
My friend replied, ‘I don’t like rice, can’t eat it. I can still eat sweetcorn but only Green Giant. Some sweetcorn tastes like shit.’ I replied, ‘Oh, that reminds me of baked beans, given up for the same reason as rice and sweetcorn.’
My friend replied, ‘I can only eat Heinz baked beans.’ I replied, ‘Was literally about to say, “and it could only be Heinz.”‘ My friend continued, ‘I can get through Tesco baked beans, but they’re not very nice.’
I continued, ‘Once, mum tried buying another brand; inedible. Same with Frankfurters, had to be Herta. She tried buying another; inedible.’ My friend replied, ‘Yes. They have this certain different taste.’
My friend continued, ‘My mum finds that when she gets a different brand to skimp or cut costs, I reject it. I will always reject as being off-tasting. I refuse to eat it, because it tastes different.’
I replied, ‘My mum was always doing that. She did it with Pepsi, refused to buy it and bought budget cola instead. I only just bore the taste.’
My friend replied, ‘I have select meals. They all need to be the same. When anything is different, I know about it. I know immediately.’ I replied, ‘Same.’
My friend continued, ‘Because I know the meals inside out. I’ve had them all hundreds of times. I know they’re all reliable. I know they can all be eaten. You’d likely be able to relate to me more on food than anyone else.’ I replied, ‘I am.’
At age 19, my friend stated:
‘I don’t like nuts or anything that is introduced into desserts. I hate when desserts are diluted with other items.’ I replied, ‘I despise nuts. Exactly, non-confectionery ones.’
My friend continued, ‘Nuts, bananas. I had an ice cream once, and it had banana slices in it, made me feel sick. It’s like how I used to hate yoghurt with bits in. Why do they do that? I hate when people make dessert, and it’s not a dessert. It ends up being savoury or non-chocolate.’
I replied, ‘Yes, or juice with bits in. It used to tickle my mouth, and I hated it.’ My friend replied, ‘Yes. I hate when I’m drinking a drink, and a substance enters my mouth.’ I replied, ‘It’s the exact kind of thing my mum would love, those nutty, fruity, bitty desserts.’
My friend continued, ‘I hate desserts that end up not being desserts, not being chocolate. Pointless. “Carrot cake”, “fruit cake”: totally pointless.’ I replied, ‘Even cheesecake is disgusting to me. Tried it once. Cheese is still a savoury food; it’s what you eat with bread or whatever.’ My friend replied, ‘Hate savoury food under the guise of being a dessert.’
My friend continued, ‘I used to hate apple crumble, especially in primary school lunches.’ I replied, ‘Always hated that. Made me feel sick, feeling this warm, mushy hot apple taste.’ My friend continued, ‘But I had one recently, and it surprised me. I had bad memories of it, but this certain one was pleasant, but it was always something I hated.’
My friend continued, ‘I’ve managed to eat a lot of vegetables now. I can eat sprouts now. I can eat certain green beans.’ I replied, ‘I never hated sprouts. It was this thing that was a trend for every child to hate, but I found them ok.’
My friend continued, ‘I can eat broccoli now; edible but not nice.’ I replied, ‘I can eat broccoli better than sprouts.’ My friend continued, ‘I can eat cauliflower sometimes. Sometimes, it has a funny taste.’
I replied, ‘Again though, it’s hit and miss. The problem with these foods is it’s too much hit and miss. My parents have sometimes got a horribly rubbery broccoli, one that literally tastes of rubber, school rubbers, but other times, it’s been really nice.
My friend continued, ‘I have a few categories: inedible, edible, good, excellent. I’d say only 2 things fall in the excellent category.’ I replied, ‘Lol, I don’t know any food that’s excellent anymore hahahaha. There’s no food that I find gorgeous anymore. Any pleasures about eating are cancelled out by the displeasures.’
My friend replied, ‘Yes; that’s why there are only 2: Irma’s garlic bread and that Lidl lamb with garlic butter.’ I replied, ‘Never liked garlic bread. I remember eating it a few times in restaurants not realising what I was eating, thinking it was just bread, and then feeling sick once I tasted it. My sister loved garlic bread, and the smell would fill the room, and I hated it.’
My friend continued, ‘I have chicken nuggets for lunch every day; reliable, edible, but not good or excellent.’ I replied, ‘Chicken nuggets are one of the most reliable foods I can eat, so I have to eat them. They rarely go wrong.’
I continued, ‘Even chips can go wrong more often than nuggets. My mum rarely buys anything but one brand of chips anymore, but when she used to, it would go wrong often. I couldn’t eat about 40% of chip brands.
That should be how I gauge food actually, percentages of how possible they are to go wrong. With broccoli, you never get the same thing; it’s always different, so the possibility of it going wrong is 100%, while the frequency, I’d say, is about 50%. Chips: they haven’t gone wrong for a long time, because my mum buys the same blue bag.
I avoid foods looking like that [restaurant chicken breast]. The less processed it looks, the more chance it has to go wrong for me. Processed can be the exact same every single time, and that’s why I like it. It complies perfectly with my Asperger’s. I’m trying desperately to finish this breakfast before I shower instead of leaving it on the plate.’
My friend replied, ‘Restaurant tends to be mostly good or edible. At home, it’s mostly in the edible category. Can’t really think of anything I enjoyed at home, other than Lidl’s lamb.’ I replied, ‘I don’t have your deal with restaurants at all, just not at all.’
I continued, ‘I’ve had far more nightmares, as a percentage, in restaurants than at home, far more. It’s gone wrong in restaurants on average way more times than it’s gone right. Often, I just couldn’t eat anything, refused to eat anything and sat quietly instead.
Overall, I hate talking about food preferences. It’s a pointless endeavour, because I’m not allowed to have them, because too much goes wrong. There are too many difficulties in the way to have preferences. There are only tolerabilities.’
At age 21, I stated:
‘Just had a whole batch of Oreo packets be absolutely fucked, taste disgusting.’ My friend replied, ‘Does it taste sweaty?’ I replied, ‘No. Honestly, the taste of these foods can be completely random sometimes. When they do go wrong, it’s usually a totally random taste.’
I continued, ‘It’s almost a smokey taste this time. It’s like I was eating a cake made of tobacco leaves and soot. Anyway, I have about 8 packets left, and don’t know how many of them are affected.
It always affects per packet and per batch, never within packets. It’s weird; you can tell which packets were made and released together or at the same plant.’
My friend replied, ‘I wonder if I would think the same if I tasted it, given that I know how they taste.’ I replied, ‘I never think about that, but yes, it’s a good question. I know my mum doesn’t.’
At age 21, I stated:
‘The fact there are established fermented drinks for basically every type of food under the sun.’ My friend replied, ‘”Ferment” has always been a negative word to me. Whenever I’ve had a fermented pineapple or apple or grape or strawberry, I’ve gagged.’ I replied, ‘Same.’
I then sent the following quote from Wikipedia: ‘Food fermentation serves five main purposes: to enrich the diet through development of a diversity of flavors, aromas, and textures in food substrates …’[23]
I remarked, ‘What the fuck sort of a reason is that? Those are the exact things I want to reduce the diversity of.’ My friend replied, ‘I hear that all the time in relation to food and don’t feel it myself. They talk about textures, aromas and flavours, but I don’t know what they’re talking about.’
My friend continued, ‘When someone is eating the same food as me, and they say all that and that it’s “beautiful”, I don’t know what they’re talking about. I genuinely don’t know. I say, “It’s just cod.”
They compliment food every single meal. I’ve only reacted like that over food about once every few years, and then they wonder why I’m not saying it myself. My mum said, “You should be saying how nice it is, how lovely it is.”‘
Pain and temperature
Both of us also have a hypersensitivity to pain and temperature.
At age 21, I stated:
‘It’s likely we have a pain and temperature hypersensitivity then. It’s never been something I had to think about, never come up consistently, but it looks like I do have one, insula-related that is.
I mentioned it because I’ve added my account of braces, in which I was extreme pain that was nothing like my sister’s, and then the fact my mum pointed out once that I reacted excessively to hot crockery in the dishwasher and said it was something my dad had.’
My friend replied, ‘Okay, yes. I know I have a pain hypersensitivity. I’ve sort of just worked it out, just because of seeing how other people react to pain compared to me.
I’ve always had a very, very, very, very low pain threshold, when I see these girls cutting their arms, and then there’s me, not even being able to stand a needle.
Mine is extremely low. There’s no way on earth that I would even be able to draw blood from my skin, and even when I’ve got to pop a spot (because it hurts, so you’ve got to pop it to make it hurt less), it’s very painful to do. You hear the noise I make afterwards; it’s an absolute grunt.’
Low weight
Both of us have significantly low weight as a result of all of the above difficulties surrounding eating, which include hypersensitivity to taste and texture and swallowing difficulties. This is in addition to an inability to see food as comfort, which is described in association with the social mindset.
I also have non-specific gastrointestinal issues resembling dysmotility that are described in a later section and also contribute to the eating difficulties in my case.
A body mass index (BMI) below 18.5 is considered underweight, while a BMI of 25 or more is considered overweight, with a BMI of 30 or more being considered obese.[24]
My BMI was within the ~50th–55th percentiles at age 5 but had dropped to the 25th percentile by age 9, where it remained until age 11, when it dropped to around the 10th percentile and then, at age 14, the 1st percentile.
Since age 14, my BMI has never left the range 14–17. However, since around age 17, my weight has tended to remain extremely stable, rarely varying more than 3 or 4 kg, and it does not follow a downward or upward trend.
As of 30 November 2020, my weight was 47 kg (BMI: 15), while my friend’s weight was 51 kg (BMI: ~16.5).
As of 30 November 2020, my all-time highest weight was 51.3 kg (BMI: 16.4), for about one week at age 19, while my friend’s all-time highest weight was 61.7 kg (BMI: ~20), at age 18.
At age 19, my friend asked what I eat and drink in a day, to which I sent a list. My friend replied:
‘2 cokes and 14 cookies haha.’ I replied, ‘It’s devolved into that since my weight issues. I used to eat fruit and everything before my weight became a problem. Now, everyone around me (dietitians, parents) has been directing me to eat high-calorie foods. My mum has purposely bought me whole milk since about 2 years ago.’
My friend replied, ‘Yes; you must. That’s what I do.’ I replied, ‘Doesn’t explain why I still had a slight calcium deficiency in my last blood test. Also, my bone density about 2 years ago was low. I’m honestly withering away as we speak.’ My friend replied, ‘Yes. It’s not good.’
RAS/MAPK pathway–related features
The RAS/MAPK signalling pathway and its involvement in autism spectrum disorder (ASD) with megalencephaly is discussed on the respective section of Genetics of our lack of the social mindset.
Although RAS/MAPK-pathway overexpression is independently associated with ASD with macrocephaly, there are a number of RAS/MAPK pathway–related syndromic conditions also associated with ASD and macrocephaly, the most relevant of which here include Noonan syndrome, Costello syndrome and cardiofaciocutaneous syndrome.
Aside from ASD and childhood macrocephaly, I have a number of mild RASopathy-like physiological features in common with these conditions, especially Noonan syndrome.
My friend has far fewer similar features. If such a mutation was involved in his condition, it may have been in a different part of the pathway to mine, leading to less pronounced features.[25]
Paternal age effect
Gain-of-function mutations in RAS/MAPK pathway–related genes are known for their significant paternal age effect, in which the risk of such a mutation in a child increases significantly with the age of the father at conception.
My father was aged 44 at my conception, while my friend’s father was aged 40 at his conception.
Posteriorly rotated, low-set ears
Posteriorly rotated, low-set ears are seen in Noonan syndrome[26] and cardiofaciocutaneous syndrome.[27]
I have mildly posteriorly rotated, mildly low-set ears, which can be seen in the image of childhood megalencephaly.

Whilst this could have been seen as a side effect of the childhood megalencephaly, it has persisted in a mild form into adulthood.
My friend does not significantly have this feature.
Micrognathia
Micrognathia (a small lower jaw) is seen in Noonan syndrome.[26]
I have mild micrognathia, which can also be seen in the image of childhood megalencephaly.
Again, despite the contribution by the childhood megalencephaly, it has persisted in a mild form into adulthood. The facial features in Noonan syndrome are noted to be most prominent in early-to-mid childhood before becoming subtle in adulthood.[28]
My friend does not have micrognathia to any significant degree.
Prominent volar pads
Prominent volar pads (also known as prominent finger pads,[29] foetal finger pads or persistent foetal fingertip pads) are seen in Noonan syndrome[26] and Costello syndrome[30] (‘spatulate finger pads’[31]).
I retain volar pads, including the three interdigital volar pads between the second-to-fifth fingers (which can be seen in this diagram).


My friend does not share this feature to any significant degree.
Café au lait macules
Café au lait macules, or patches of hyperpigmentation due to a local overabundance of melanocytes, are seen in Noonan syndrome[26] and neurofibromatosis type 1.[32]
I have two known café au lait macules, while my friend has one known café au lait macule.
Around 20% of people have at least one café au lait macule (though less so in white populations),[33] so they carry little significance on their own, though the constellation of symptoms may render them clinically related.
Gastrointestinal issues
Gastrointestinal issues resembling dysmotility, contributing to inadequate weight gain, are seen in Noonan syndrome,[34] Costello syndrome[31] and cardiofaciocutaneous syndrome.[35]
In addition to all of the aforementioned eating difficulties, I have also had non-specific gastrointestinal issues resembling dysmotility since earliest memories.
Throughout life, I have become fuller much more quickly than my family. Eating past this point would always result in nausea, though I always avoided vomiting.
I was seen by doctors for these issues beginning at around age 10 and was diagnosed with ‘chronic habitual constipation’. Following this, I was seen by growth specialists and dietitians until around age 17.
My friend does not have similar gastrointestinal issues but retains other eating issues such as those related to swallowing.
At age 21, I stated:
‘[It] starts only after putting food in the mouth. [The digestive system] then becomes blocked. I feel like I cannot swallow it for the life of me when this issue occurs. It doesn’t start before eating; it only becomes an issue after the first mouthful.
There suddenly becomes a blockage. I try to brave through it, but I end up feeling movements in my lower bowels and having to suddenly stand up.’
Growth and delayed puberty
Delayed puberty is seen in paternal-age-effect conditions/RASopathies such as Noonan syndrome[36] (in which one study reported a 2-year delay[37]).
My puberty was delayed by about 2 years. My MRI at age 14 was carried out as a result of growth delays. It revealed a reduced size of the pituitary gland, and consequently, this was the only finding it reported as potentially significant.
The following is a sagittal MRI slice of my pituitary gland compared to one from the closest available male reference MRI in age (20) on Radiopaedia for which a clear sagittal view was available. The MRIs are not to scale.

Source: [38]. Licence: CC-BY-NC-SA-3.0.

My pituitary gland can also be compared against the following available sagittal reference MRIs on Radiopaedia. All show a similar difference:
Male:
Female:
Unknown sex:
At age 5, my height was at around the 50th percentile, but by age 7, it had fallen to around the 25th percentile, and I was among the shortest in the class in all schools from around age 5 onwards.
My height remained in the region of the 25th percentile right up until expected puberty (which I missed), when it dropped to roughly the 6th–8th percentile (151 cm) at age 14 before rising to roughly the 45th percentile (175 cm) at age 17.5. By age 20, my height had reached the 50th–55th percentile (177.5 cm).
Other than delayed puberty, I have had several symptoms that could be suggestive of hypopituitarism,[39][40] including osteopenia, symptoms of exertional hypotension and idiopathic postprandial syndrome and less androgenic body hair than my friend, however some may have been contributed to by the eating difficulties and low weight.
Additionally, despite the small pituitary size, a 2019 blood test showed a normal level of thyroid-stimulating hormone (1.95 mU/L; reference range: 0.3–5.0), and I am unaware of any requested blood test having measured and reported low levels of pituitary hormones.
Due to lacking an MRI for my friend, I am unable to provide his pituitary size, however he has not had significant symptoms suggestive of hypopituitarism. He has reported that he was also among the shortest in the class before puberty, however his puberty was at an average age.
Noonan syndrome,[26][36] cardiofaciocutaneous syndrome[35] and delayed puberty[41] often result in a short final adult height. However, as mentioned, after my pubertal growth spurt, which was during the latter half of age 15 to age 16, I reached just above exactly average height.
Noonan syndrome and Noonan syndrome with multiple lentigines (LEOPARD syndrome) also often result in symptoms of genital underdevelopment, such as cryptorchidism[42] or hypospadias.[43] Neither of us have this, and I have instead had the converse (overdevelopment).
Family history
There is a significant contribution of my paternal family history to my condition. A contribution from my friend’s paternal family history to his condition is possible but less apparent.
In contrast, there appears to be no apparent contribution of our maternal family histories to our condition.
Paternal
My father significantly retains the social mindset but has autistic features. Almost all of my features are gross accentuations of his.
Although never diagnosed with an autism spectrum disorder, he dislikes interference with his order of things and has mildly clumsy fine-motor movements. He was an engineer/manager for a national defence firm, and his mother was a member of Mensa.
My friend has not reported significant autistic features in his father, however his father also worked for an engineering firm and shares knowledge about computers and electronics with him.
Maternal
Our mothers do not appear to have contributed to our condition.
Both of them have a histrionic personality that is generally polar to ourselves. Both show highly exaggerated emotions and vocal intonation, and both have a propensity to become very emotionally worked over a seemingly minor issue, often to the point of screaming and swearing.
My friend has reported that his mother apparently imposes factitious disorders on both herself and him and suggests that either she or he will die due to various benign reasons. My mother has often considered that many benign or common conditions that I have acquired (such as a stye or paronychia) will lead to a grave outcome or death and are my fault. My friend has described his mother as ‘scheming’ in order to get her way with authority figures, and this also describes my mother.
Although undocumented in medical literature, there may be a phenomenon in which males with autistic traits end up with females with borderline or histrionic traits at a much higher rate than average. There are anecdotal reports online of this.[44]
When I increasingly reduced my effort to speak to potential partners after age 15, I noticed an increasingly larger portion of those who did engage having these traits, at least two of whom mentioned having had an unusually large proportion of partners with high-functioning autism in the past. My friend has also been told this by at least one girl he spoke to who was diagnosed with borderline personality disorder.
I believe the phenomenon to be primarily due to the relative lack of initiation by males with autistic traits and the relatively high degree of initiation by females with these traits. The lack of initiation by males with autistic traits has also been put forward as a contributing factor for the high age of fathers with autistic children.[45]
Siblings
Both of us have either siblings or half-siblings who are unaffected by our condition.
References
- ^ "Language Milestones 1 to 2 Years: First Words, Gestures, and More". Healthline. 2018-06-12. (Archive version from 18 July 2020.)
- ^ "Number Memory - Human Benchmark". humanbenchmark.com. (Archive version from 19 September 2020.)
- ^ "Verbal Memory - Human Benchmark". humanbenchmark.com. (Archive version from 4 October 2020.)
- ^ Leonard, Kimberlee (2019-01-29). "What Is a Good Typing Speed Per Minute?" Small Business - Chron.com. (Archive version from 18 September 2020.)
- ^ a b American Psychiatric Association (2013-05-22). "Diagnostic and Statistical Manual of Mental Disorders (5th ed.)".
- ^ "ICD-10 Version:2016". icd.who.int.
- ^ a b Bloch, Michael H.; Landeros-Weisenberger, Angeli; Rosario, Maria C.; Pittenger, Christopher; Leckman, James F (2008-12). "Meta-Analysis of the Symptom Structure of Obsessive-Compulsive Disorder". The American journal of psychiatry. PubMed Central. 165 (12): 1532–1542. doi:10.1176/appi.ajp.2008.08020320. ISSN 0002-953X. PMC 3972003. PMID 18923068.
- ^ "OCD - Symptoms". nhs.uk. 2018-06-19. (Archive version from 6 August 2020.)
- ^ a b "Insistence on Sameness | Interactive Autism Network". iancommunity.org. 2007-04-02. (Archive version from 10 September 2020.)
- ^ a b c Brock, Hannah; Hany, Manassa (2020). "Obsessive-Compulsive Disorder (OCD)". PMID 31985955.
- ^ Leopold, Rebecca; Backenstrass, Matthias (2015-03-01). "Neuropsychological differences between obsessive-compulsive washers and checkers: A systematic review and meta-analysis". Journal of Anxiety Disorders. ScienceDirect. 30: 48–58. doi:10.1016/j.janxdis.2014.12.016. ISSN 0887-6185.
- ^ "Obsessive-compulsive disorder (OCD) - Symptoms and causes". Mayo Clinic. (Archive version from 25 August 2020.)
- ^ a b Stevens, Francis L.; Hurley, Robin A.; Taber, Katherine H.; Hurley, Robin A.; Hayman, L. Anne; Taber, Katherine H (2011-04-01). "Anterior Cingulate Cortex: Unique Role in Cognition and Emotion". The Journal of Neuropsychiatry and Clinical Neurosciences. 23 (2): 121–125. doi:10.1176/jnp.23.2.jnp121. ISSN 0895-0172.
- ^ Ghaziuddin, M.; Butler, E (1998). "Clumsiness in autism and Asperger syndrome: a further report". Journal of Intellectual Disability Research. 42 (1): 43–48. doi:10.1046/j.1365-2788.1998.00065.x. ISSN 1365-2788.
- ^ C. N. X. OpenStax (2016-05-27). "Different parts of the motor cortex control different muscle groups. Muscle groups that are neighbors in the body are generally controlled by neighboring regions of the motor cortex as well. For example, the neurons that control finger movement are near the neurons that control hand movement." Wikimedia Commons.
- ^ Lewin, Adam B.; Chang, Susanna; McCracken, James; McQueen, Melissa; Piacentini, John (2010-07-30). "Comparison of clinical features among youth with tic disorders, obsessive–compulsive disorder (OCD), and both conditions". Psychiatry Research. 178 (2): 317–322. doi:10.1016/j.psychres.2009.11.013. ISSN 0165-1781.
- ^ Darrow, Sabrina M.; Grados, Marco; Sandor, Paul; Hirschtritt, Matthew E.; Illmann, Cornelia; Osiecki, Lisa; Dion, Yves; King, Robert; Pauls, David; Budman, Cathy L.; Cath, Danielle C.; Greenberg, Erica; Lyon, Gholson J.; McMahon, William M.; Lee, Paul C.; Delucchi, Kevin L.; Scharf, Jeremiah M.; Mathews, Carol A (2017-7). "Autism Spectrum Symptoms in a Tourette Syndrome Sample". Journal of the American Academy of Child and Adolescent Psychiatry. 56 (7): 610–617.e1. doi:10.1016/j.jaac.2017.05.002. ISSN 0890-8567. PMC 5648014. PMID 28647013.
- ^ Weeks, R. A.; Turjanski, N.; Brooks, D. J (1996-06-01). "Tourette's syndrome: a disorder of cingulate and orbitofrontal function?" QJM: An International Journal of Medicine. 89 (6): 401–408. doi:10.1093/qjmed/89.6.401. ISSN 1460-2725.
- ^ DeLong, Mahlon; Wichmann, Thomas (2010-4). "Changing Views of Basal Ganglia Circuits and Circuit Disorders". Clinical EEG and neuroscience. 41 (2): 61–67. ISSN 1550-0594. PMC 4305332. PMID 20521487.
- ^ Leckman, James F.; Zhang, Heping; Vitale, Amy; Lahnin, Fatima; Lynch, Kimberly; Bondi, Colin; Kim, Young-Shin; Peterson, Bradley S (1998-07-01). "Course of Tic Severity in Tourette Syndrome: The First Two Decades". Pediatrics. 102 (1): 14–19. doi:10.1542/peds.102.1.14. ISSN 0031-4005, 1098-4275. PMID 9651407.
- ^ Robertson, Mary May; Eapen, Valsamma (2014-10-01). "Tourette's: Syndrome, disorder or spectrum? Classificatory challenges and an appraisal of the DSM criteria". Asian Journal of Psychiatry. 11: 106–113. doi:10.1016/j.ajp.2014.05.010. ISSN 1876-2018.
- ^ "The violent attack that turned a man into a maths genius". BBC Future. 2019-04-11. (Archive version from 20 August 2020.)
- ^ "Fermentation in food processing". Wikipedia. 2020-09-25.
- ^ "WHO | Mean Body Mass Index (BMI)". WHO. (Archive version from 15 September 2020.)
- ^ Bentires-Alj, Mohamed; Kontaridis, Maria I.; Neel, Benjamin G (2006-03). "Stops along the RAS pathway in human genetic disease". Nature Medicine. 12 (3): 283–285. doi:10.1038/nm0306-283. ISSN 1546-170X.
- ^ a b c d e van der Burgt, Ineke (2007-01-14). "Noonan syndrome". Orphanet Journal of Rare Diseases. 2: 4. doi:10.1186/1750-1172-2-4. ISSN 1750-1172. PMC 1781428. PMID 17222357.
- ^ Pierpont, Mary Ella M.; Magoulas, Pilar L.; Adi, Saleh; Kavamura, Maria Ines; Neri, Giovanni; Noonan, Jacqueline; Pierpont, Elizabeth I.; Reinker, Kent; Roberts, Amy E.; Shankar, Suma; Sullivan, Joseph; Wolford, Melinda; Conger, Brenda; Santa Cruz, Molly; Rauen, Katherine A (2014-10). "Cardio-Facio-Cutaneous Syndrome: Clinical Features, Diagnosis, and Management Guidelines". Pediatrics. 134 (4): e1149–e1162. doi:10.1542/peds.2013-3189. ISSN 0031-4005. PMC 4179092. PMID 25180280.
- ^ Romano, Alicia A.; Allanson, Judith E.; Dahlgren, Jovanna; Gelb, Bruce D.; Hall, Bryan; Pierpont, Mary Ella; Roberts, Amy E.; Robinson, Wanda; Takemoto, Clifford M.; Noonan, Jacqueline A (2010-10-01). "Noonan Syndrome: Clinical Features, Diagnosis, and Management Guidelines". Pediatrics. 126 (4): 746–759. doi:10.1542/peds.2009-3207. ISSN 0031-4005, 1098-4275. PMID 20876176.
- ^ "Prominent fingertip pads (Concept Id: C1835807) - MedGen - NCBI". www.ncbi.nlm.nih.gov.
- ^ Lehalle, Daphne; Williams, Charles; Siu, Victoria Mok; Clayton‐Smith, Jill (2011). "Fetal pads as a clue to the diagnosis of Pitt–Hopkins syndrome". American Journal of Medical Genetics Part A. 155 (7): 1685–1689. doi:10.1002/ajmg.a.34055. ISSN 1552-4833.
- ^ a b Gripp, Karen W.; Rauen, Katherine A.; Adam, Margaret P.; Ardinger, Holly H.; Pagon, Roberta A.; Wallace, Stephanie E.; Bean, Lora JH; Stephens, Karen; Amemiya, Anne (1993). "Costello Syndrome". PMID 20301680.
- ^ Friedman, J. M.; Adam, Margaret P.; Ardinger, Holly H.; Pagon, Roberta A.; Wallace, Stephanie E.; Bean, Lora JH; Stephens, Karen; Amemiya, Anne (1993). "Neurofibromatosis 1". PMID 20301288.
- ^ Landau, Marina; Krafchik, Bernice R (1999-06-01). "The diagnostic value of café-au-lait macules". Journal of the American Academy of Dermatology. 40 (6): 877–890. doi:10.1016/S0190-9622(99)70075-7. ISSN 0190-9622, 1097-6787.
- ^ Gupta, Rishi; Chogle, Ashish; Bhangoo, Amrit (2019-01-01). "Chapter 6 - Gastrointestinal Manifestations of Noonan Syndrome". 85–91.
- ^ a b Roberts, A; Allanson, J; Jadico, S K; Kavamura, M I; Noonan, J; Opitz, J M; Young, T; Neri, G (2006-11). "The cardiofaciocutaneous syndrome". Journal of Medical Genetics. 43 (11): 833–842. doi:10.1136/jmg.2006.042796. ISSN 0022-2593. PMC 2563180. PMID 16825433.
- ^ a b Noonan, Jacqueline A (2006-12). "Noonan syndrome and related disorders: Alterations in growth and puberty". Reviews in Endocrine & Metabolic Disorders. 7 (4): 251–255. doi:10.1007/s11154-006-9021-1. ISSN 1389-9155. PMC 1894828. PMID 17177115.
- ^ Ranke, M. B.; Heidemann, P.; Knupfer, C.; Enders, H.; Schmaltz, A. A.; Bierich, J. R (1988-12-01). "Noonan syndrome: growth and clinical manifestations in 144 cases". European Journal of Pediatrics. 148 (3): 220–227. doi:10.1007/BF00441408. ISSN 1432-1076.
- ^ Case contributed by Assoc Prof Frank Gaillard. "Normal brain MRI (non-focal epilepsy protocol) | Radiology Case | Radiopaedia.org". Radiopaedia.
- ^ Schneider, Harald Jörn; Aimaretti, Gianluca; Kreitschmann-Andermahr, Ilonka; Stalla, Günter-Karl; Ghigo, Ezio (2007-04-28). "Hypopituitarism". The Lancet. 369 (9571): 1461–1470. doi:10.1016/S0140-6736(07)60673-4. ISSN 0140-6736, 1474-547X. PMID 17467517.
- ^ van Aken, M. O.; Lamberts, S. W. J (2005-12-01). "Diagnosis and Treatment of Hypopituitarism: An Update". Pituitary. 8 (3): 183–191. doi:10.1007/s11102-006-6039-z. ISSN 1573-7403.
- ^ Rohani, Farzaneh; Alai, Mohammad Reza; Moradi, Sedighe; Amirkashani, Davoud (2018-02-19). "Evaluation of near final height in boys with constitutional delay in growth and puberty". Endocrine Connections. 7 (3): 456–459. doi:10.1530/EC-18-0043. ISSN 2049-3614. PMC 5854851. PMID 29459422.
- ^ Digilio, MC; Marino, B (2001). "Clinical manifestations of Noonan syndrome". Images in Paediatric Cardiology. 3 (2): 19–30. ISSN 1729-441X. PMC 3232501. PMID 22368597.
- ^ Gelb, Bruce D.; Tartaglia, Marco; Adam, Margaret P.; Ardinger, Holly H.; Pagon, Roberta A.; Wallace, Stephanie E.; Bean, Lora JH; Stephens, Karen; Amemiya, Anne (1993). "Noonan Syndrome with Multiple Lentigines". PubMed. PMID 20301557.
- ^ "r/aspergers - Aspie guys & BPD women". reddit. (Archive version from 10 September 2020.)
- ^ Hultman, C. M.; Sandin, S.; Levine, S. Z.; Lichtenstein, P.; Reichenberg, A (2011-12). "Advancing paternal age and risk of autism: new evidence from a population-based study and a meta-analysis of epidemiological studies". Molecular Psychiatry. 16 (12): 1203–1212. doi:10.1038/mp.2010.121. ISSN 1476-5578.
- ^ "Number Memory - Human Benchmark". humanbenchmark.com. (Archive version from 19 September 2020.)
{kind=link}